

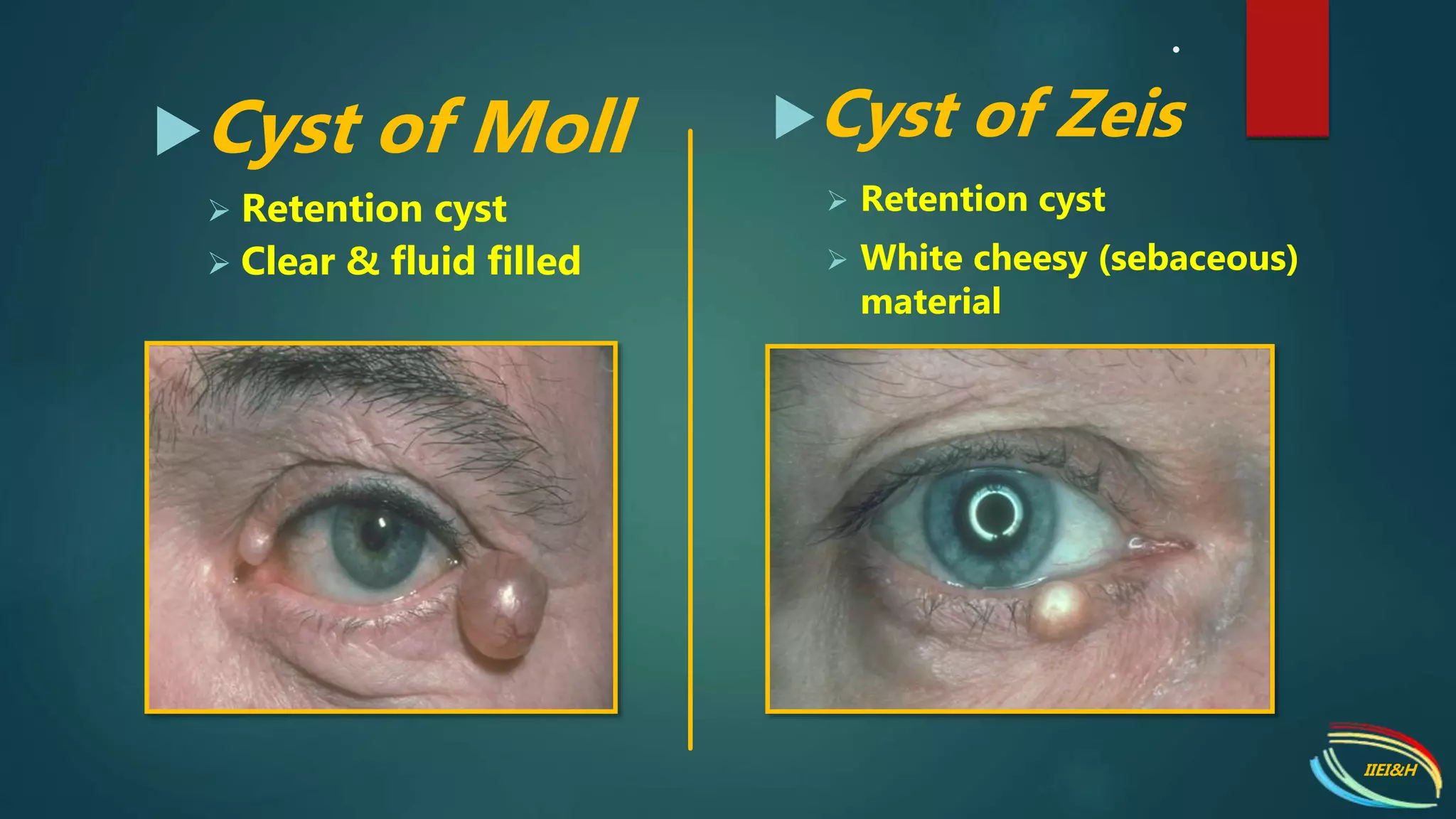

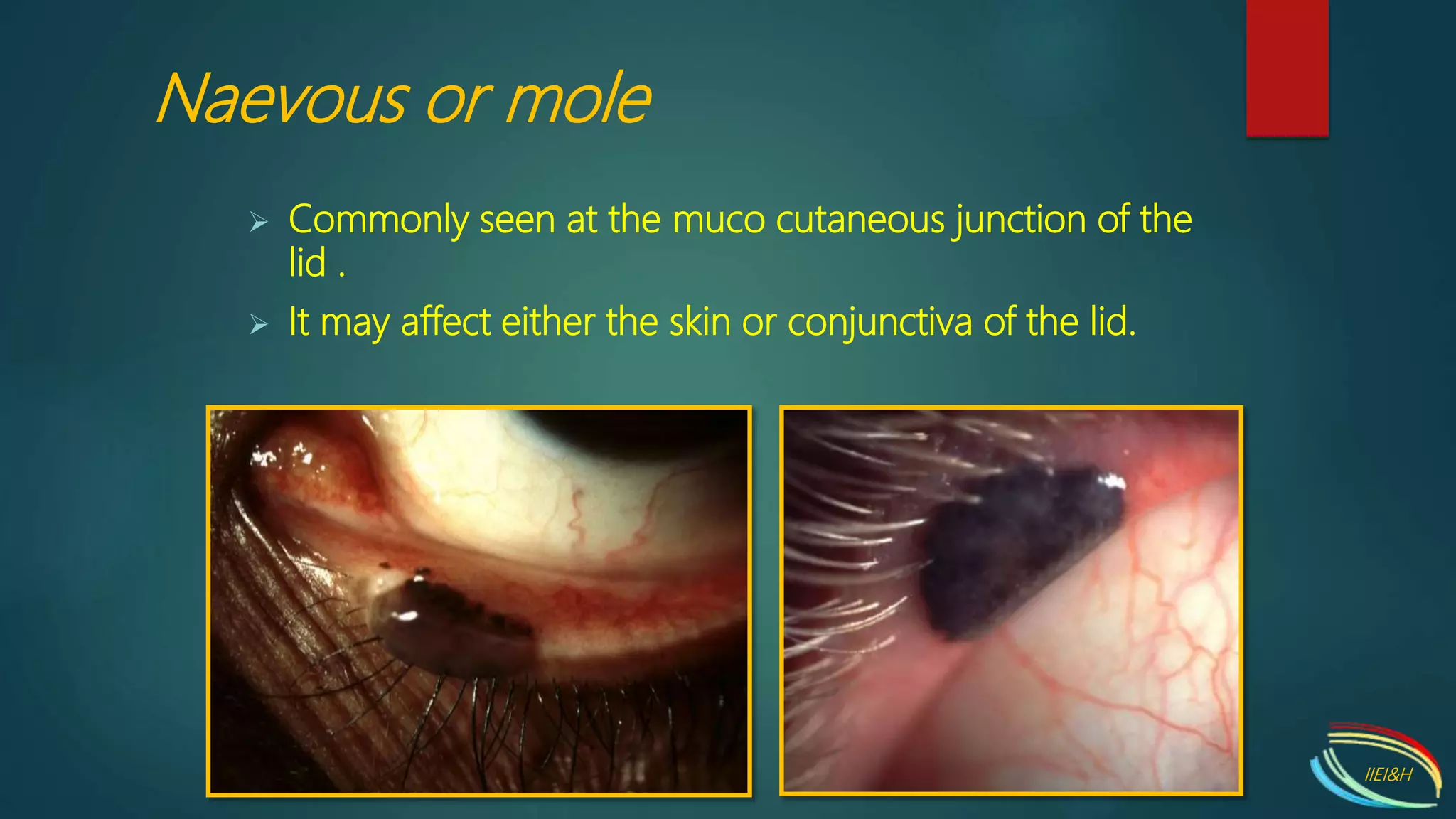
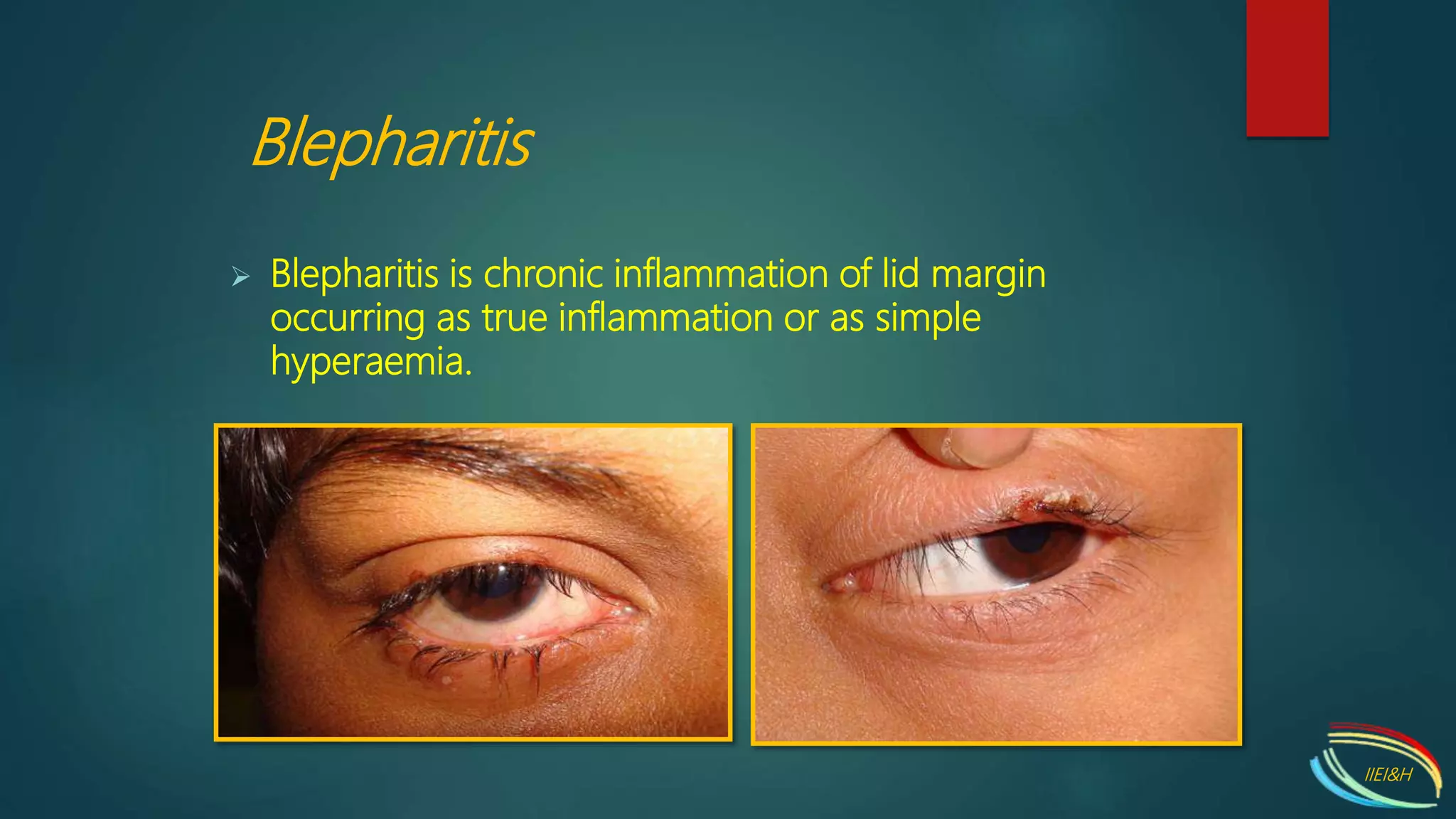



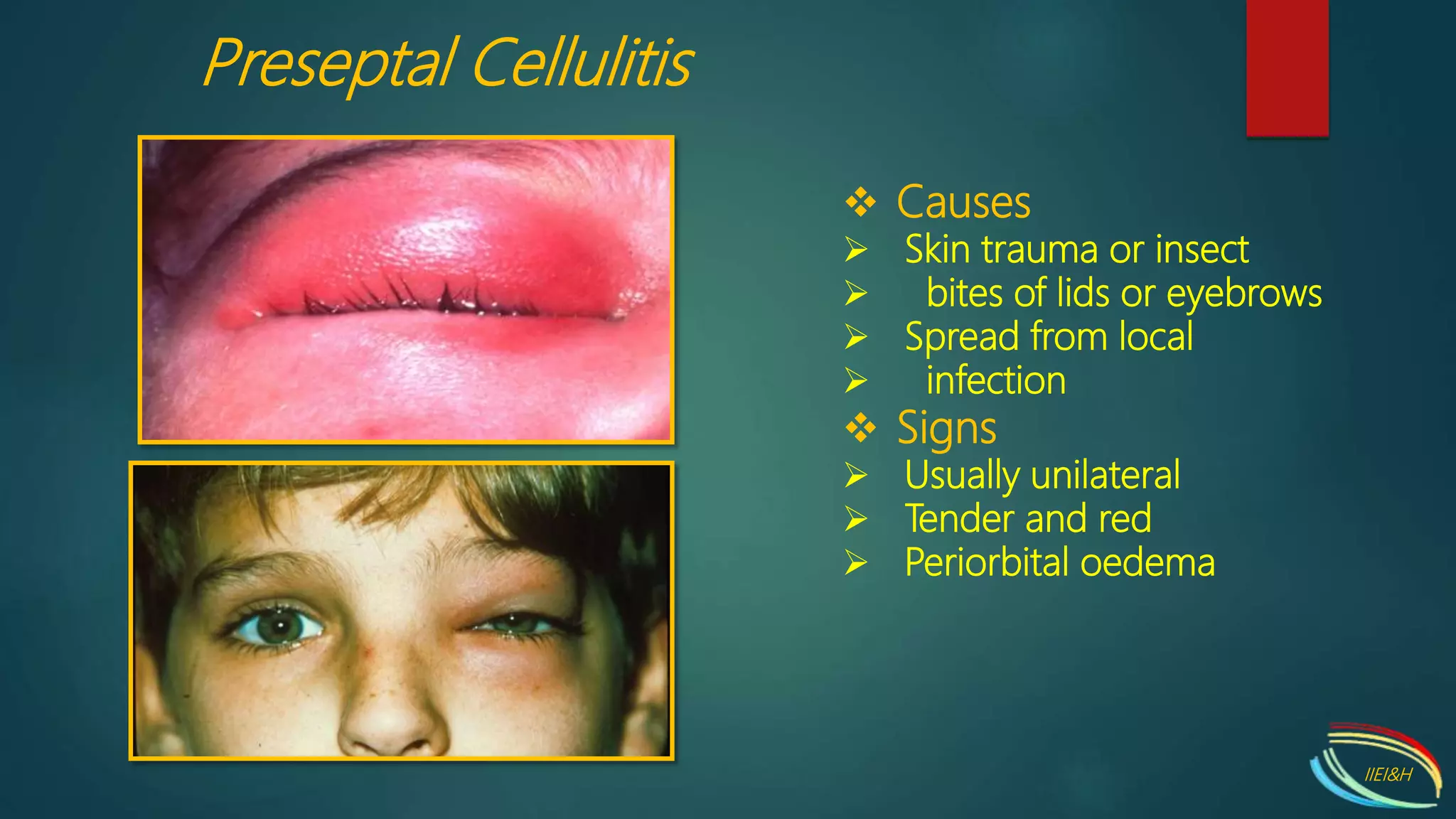



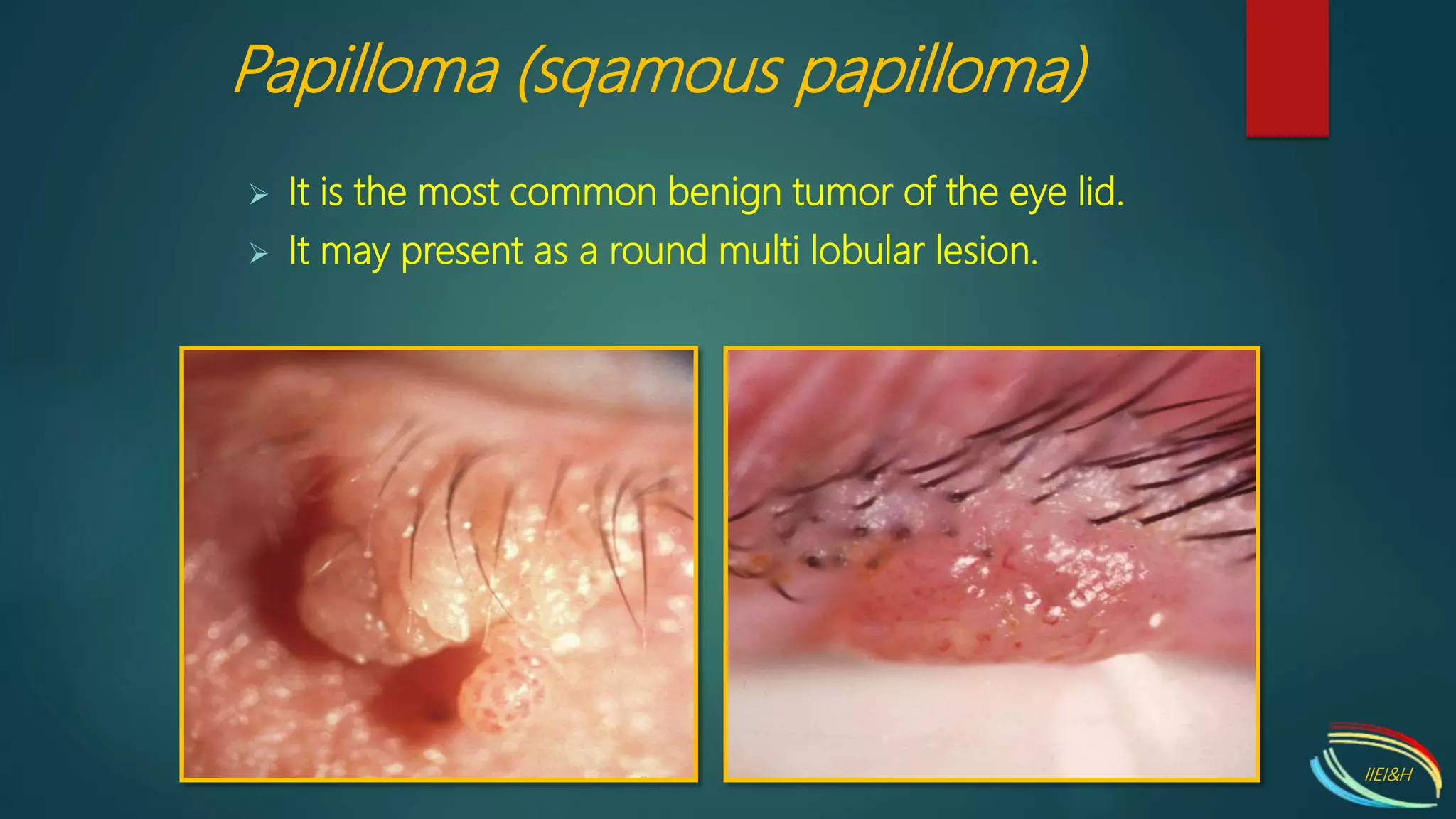




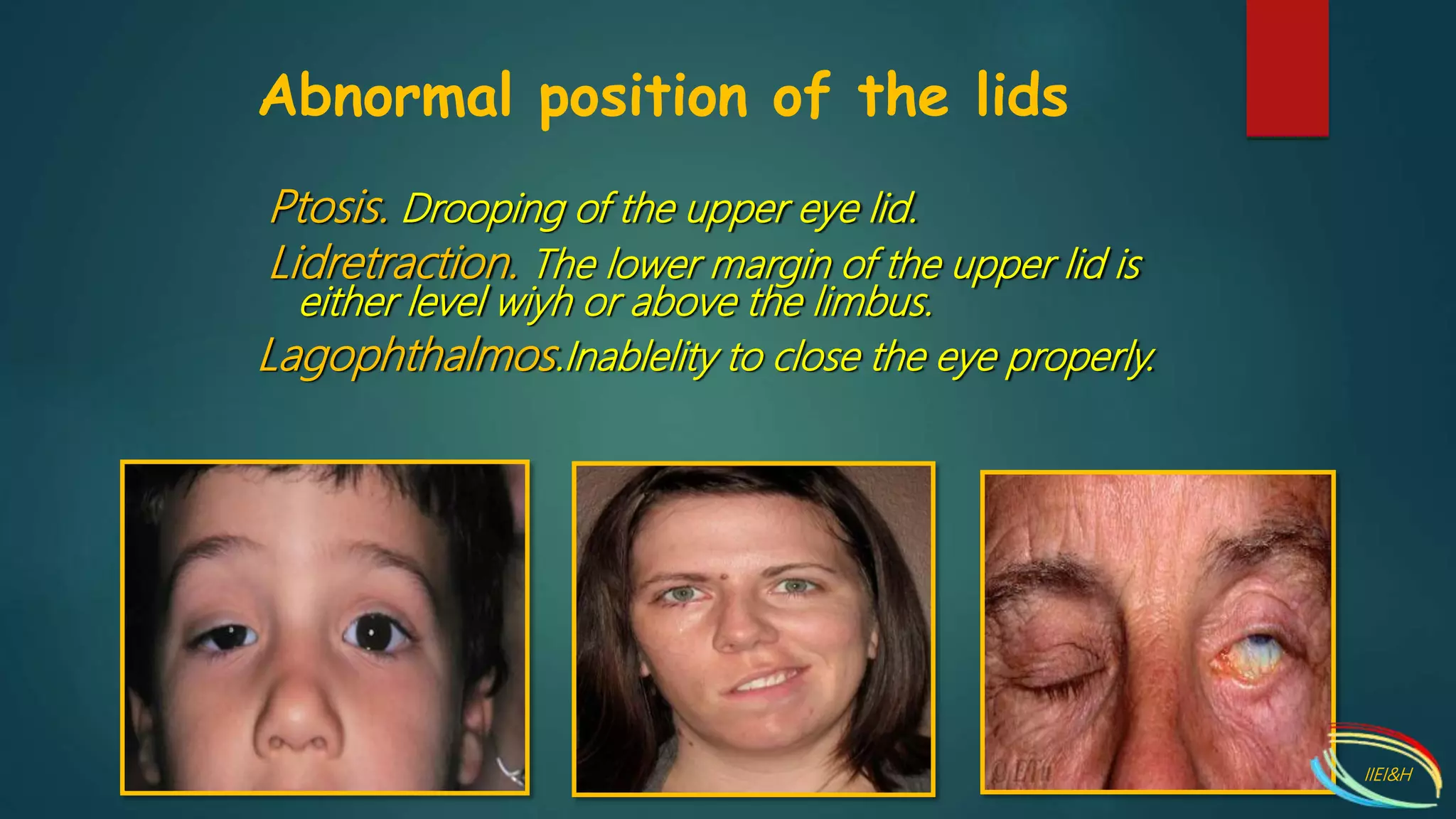




This document summarizes various clinical features of lid disorders including nodules, cysts, tumors, infections, malpositions, and traumatic injuries. It describes conditions such as chalazion, hordeolum, molluscum, xanthelasma, blepharitis, herpes, entropion, ectropion, and ptosis. It also lists systemic causes of lid edema and malignant conditions that can affect the lids.























































































