Downloaded 21 times

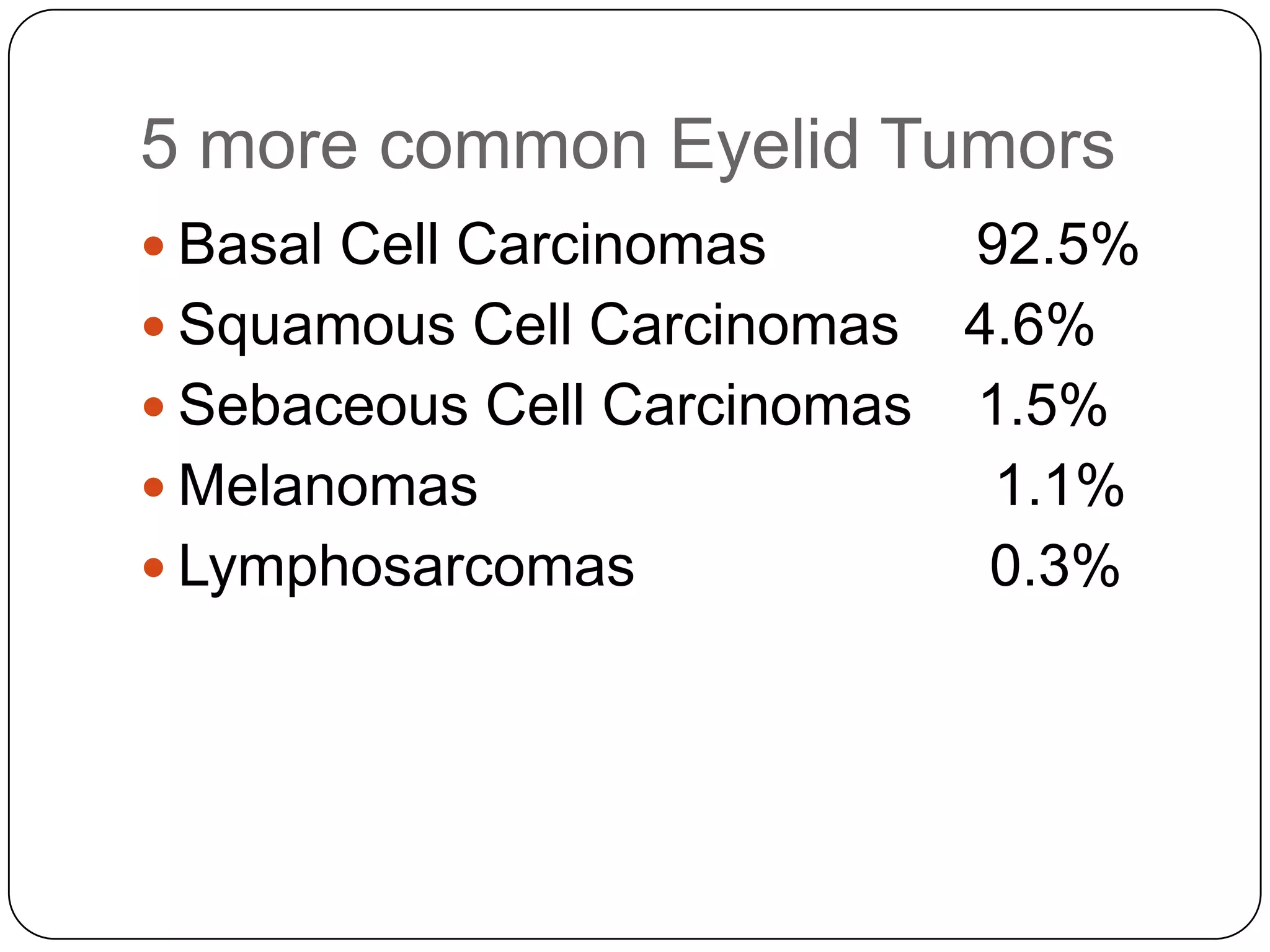

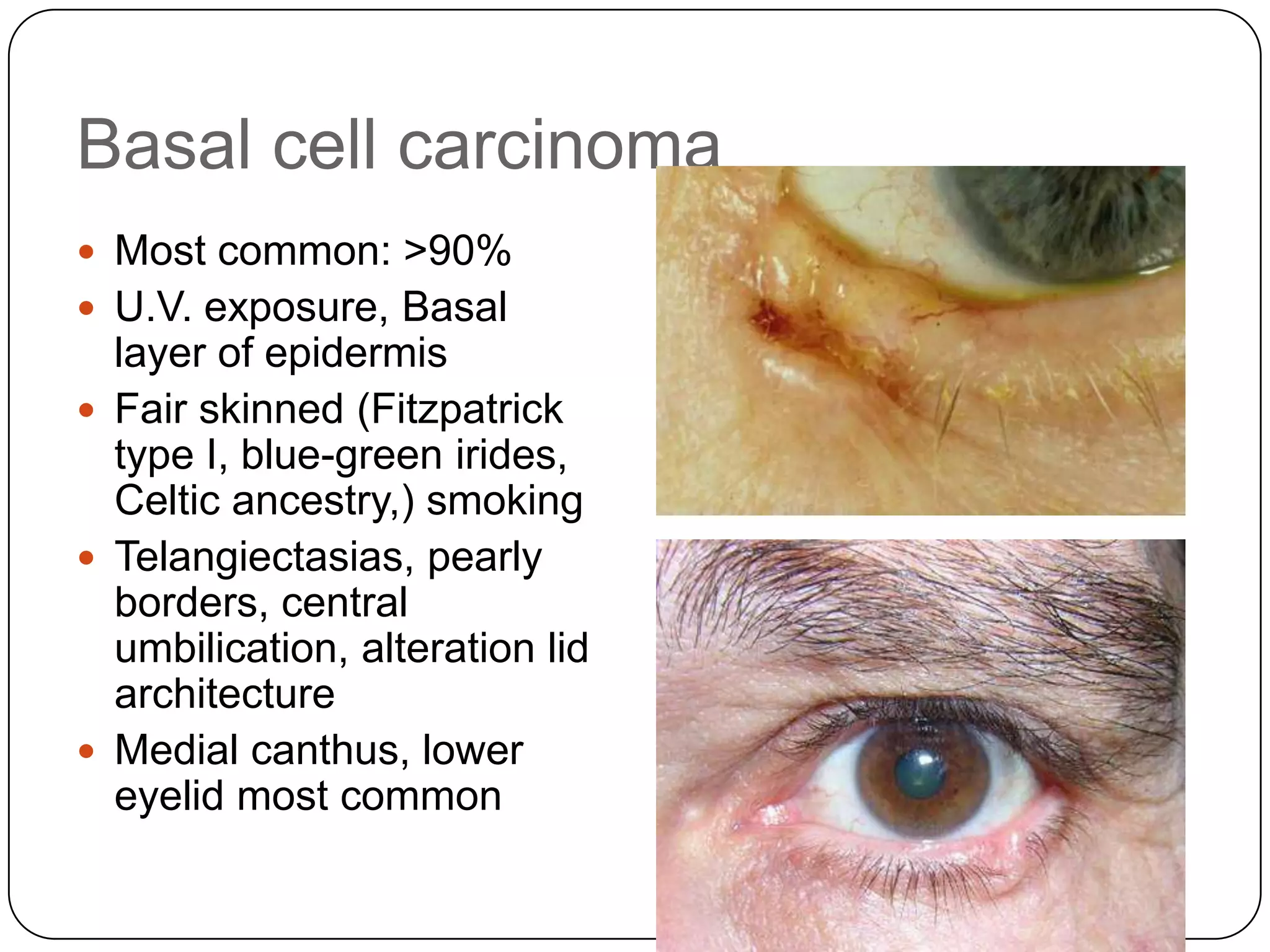







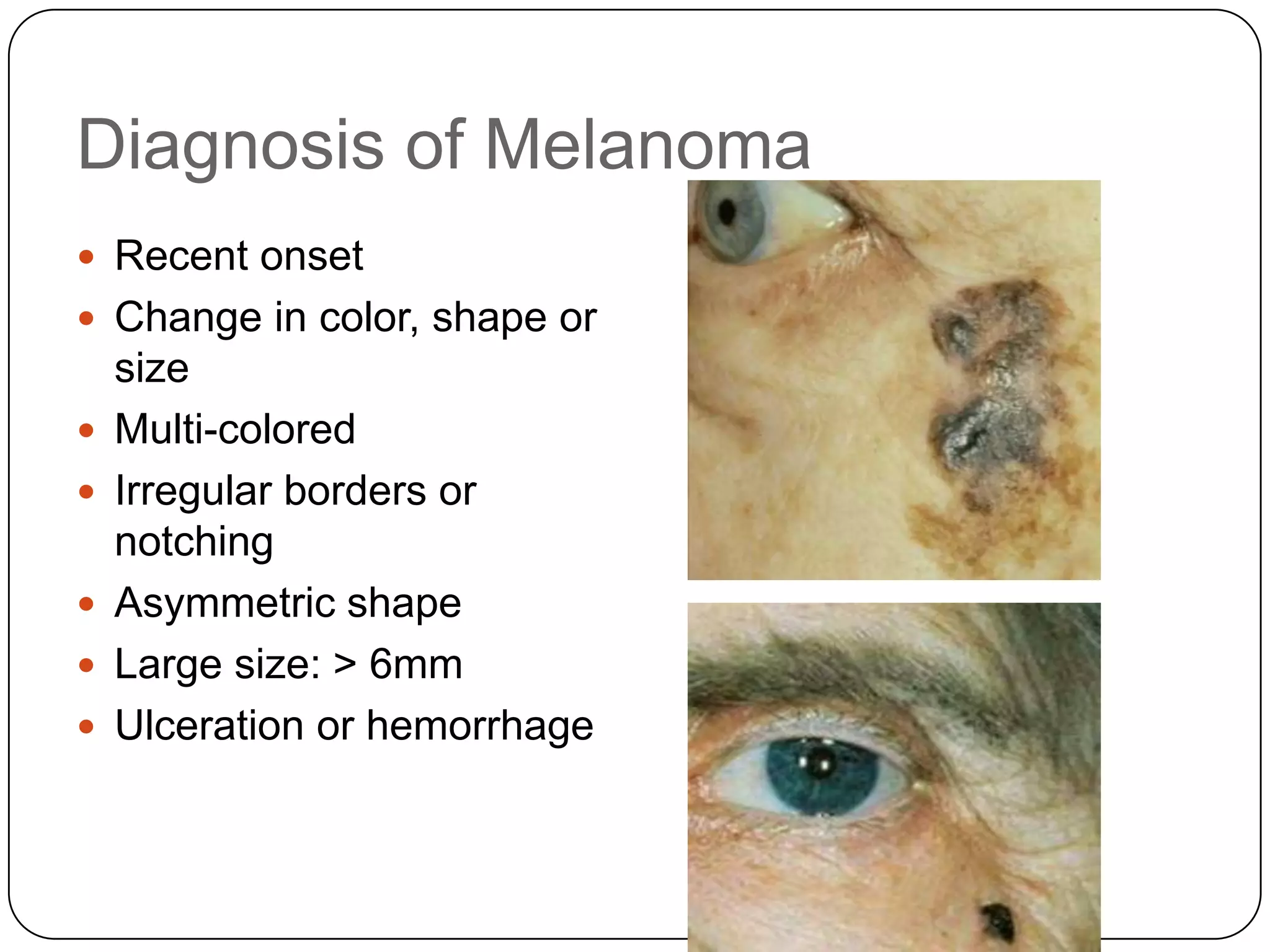































The document reviews ocular malignancies of the eyelids, cornea, conjunctiva, and iris. It discusses the most common eyelid tumors including basal cell carcinomas, squamous cell carcinomas, sebaceous cell carcinomas, and melanomas. It also reviews conjunctival intraepithelial neoplasia, invasive squamous cell carcinoma of the conjunctiva, and less common conjunctival neoplasms. Finally, it discusses tumors of the iris including nevi, melanomas, and other benign and malignant lesions.



































































