
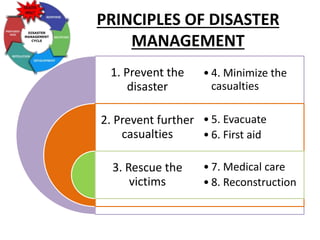

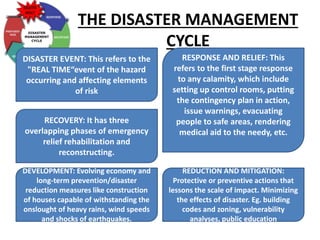
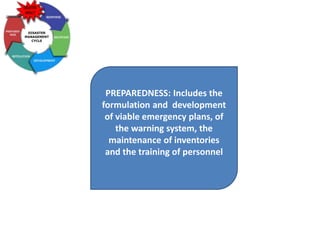
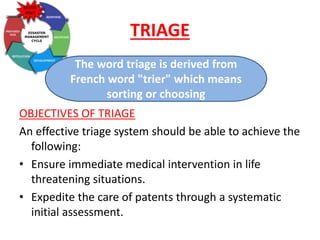





The document presents a comprehensive overview of disaster management, defining disasters, classifying them into natural and man-made types, and outlining principles of disaster management. Key components include preparedness, response, recovery, and the role of healthcare professionals in triage and community support during and after disasters. It also emphasizes the importance of hospital disaster plans and community involvement in disaster preparedness and recovery efforts.























































































