Downloaded 622 times


















![Nerve Supply
Innervation of the tongue
consists of motor fibers,
special sensory fibers for
taste, and general sensory
fibers for sensation.
Taste and general
sensation from the
pharyngeal part of the
tongue are carried by the
glossopharyngeal nerve
[IX] .
Mujtaba Ashraf 25](https://image.slidesharecdn.com/developmentoftongue-160814075631/75/Development-of-tongue-Speech-Prosthodontic-consideration-25-2048.jpg)
![Mujtaba Ashraf 26
General sensory
innervation from the
anterior two-thirds or
oral part of the tongue is
carried by the lingual
nerve, which is a major
branch of the
mandibular nerve [V 3] .](https://image.slidesharecdn.com/developmentoftongue-160814075631/75/Development-of-tongue-Speech-Prosthodontic-consideration-26-2048.jpg)














































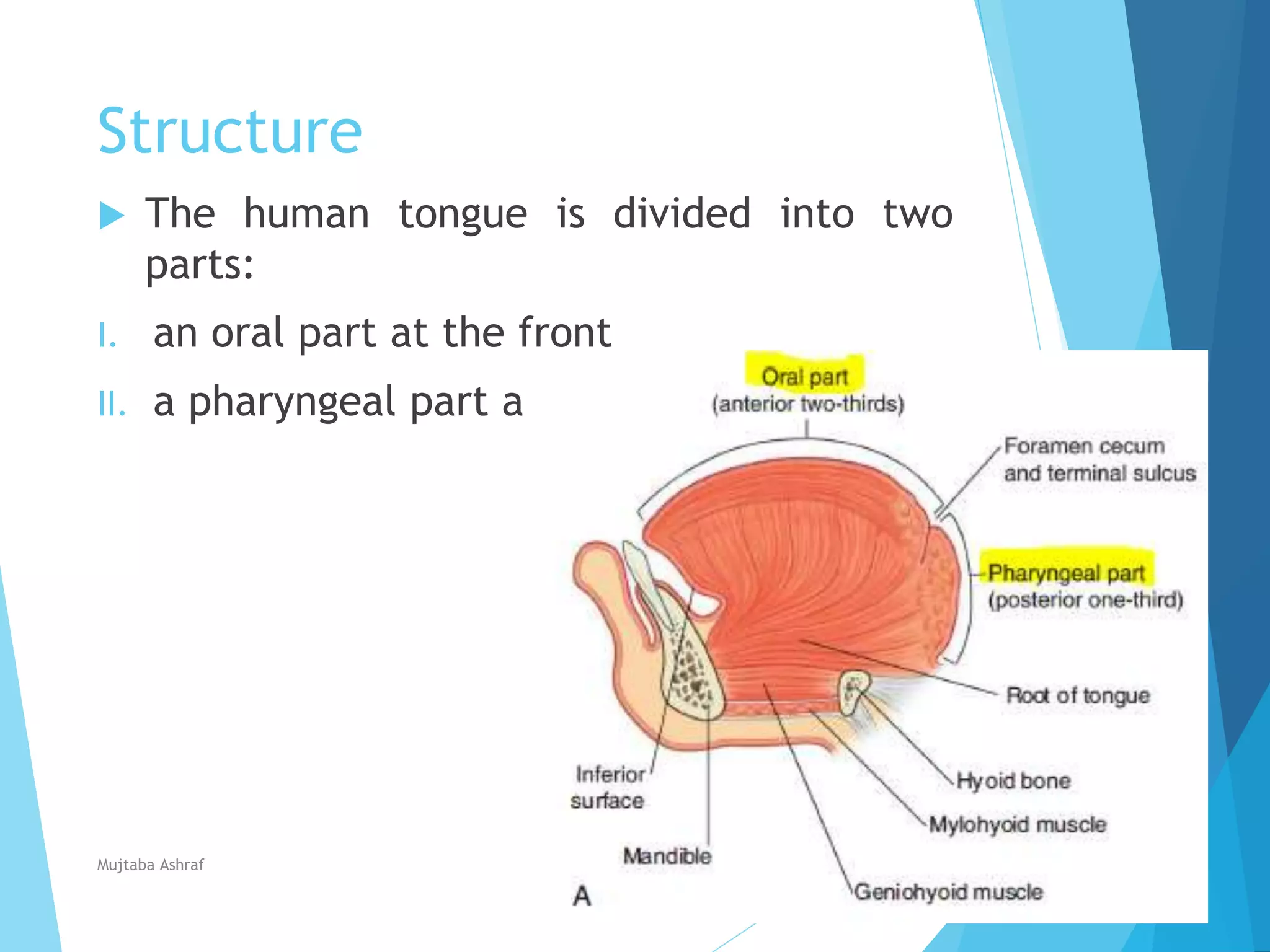
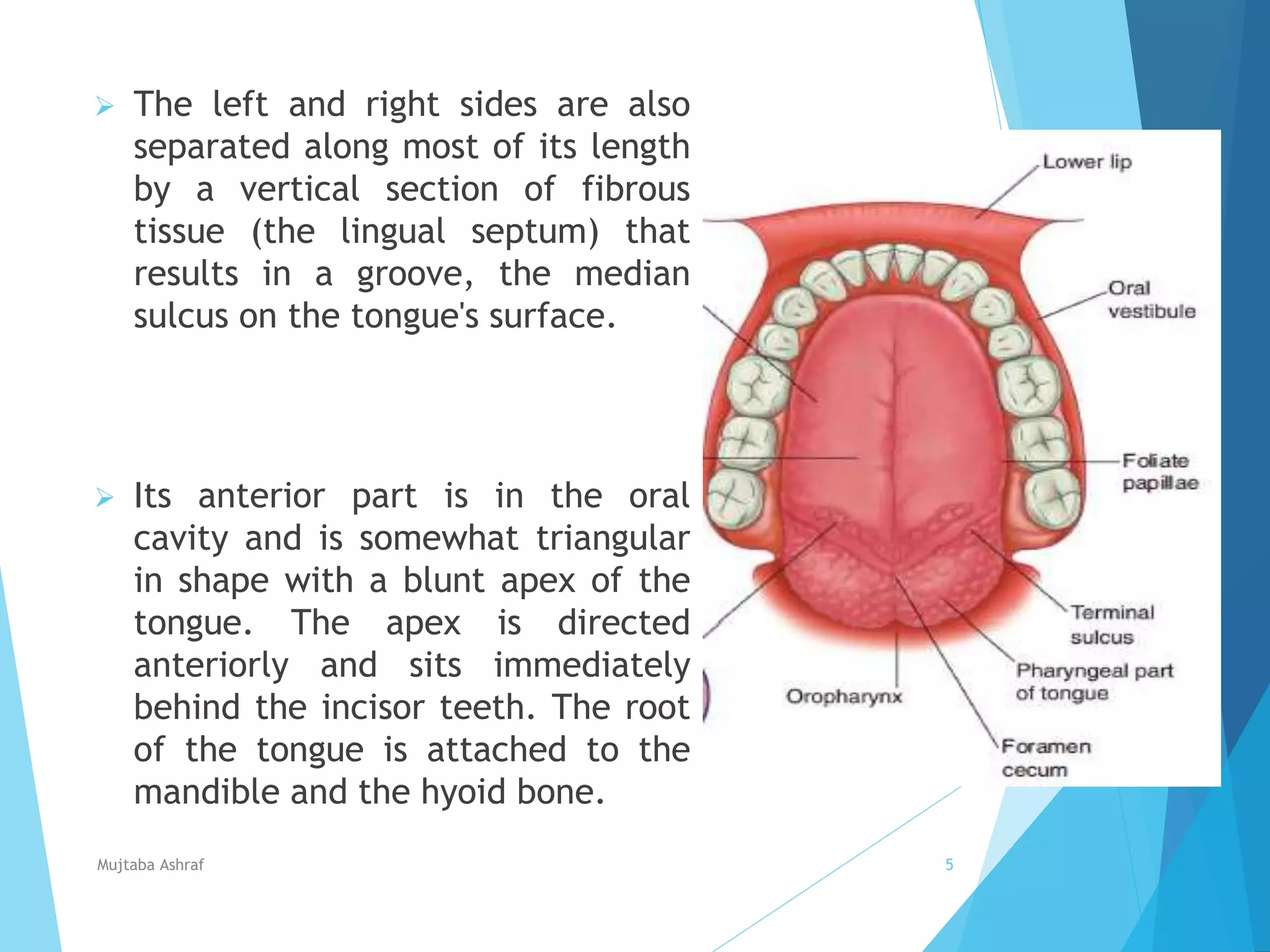
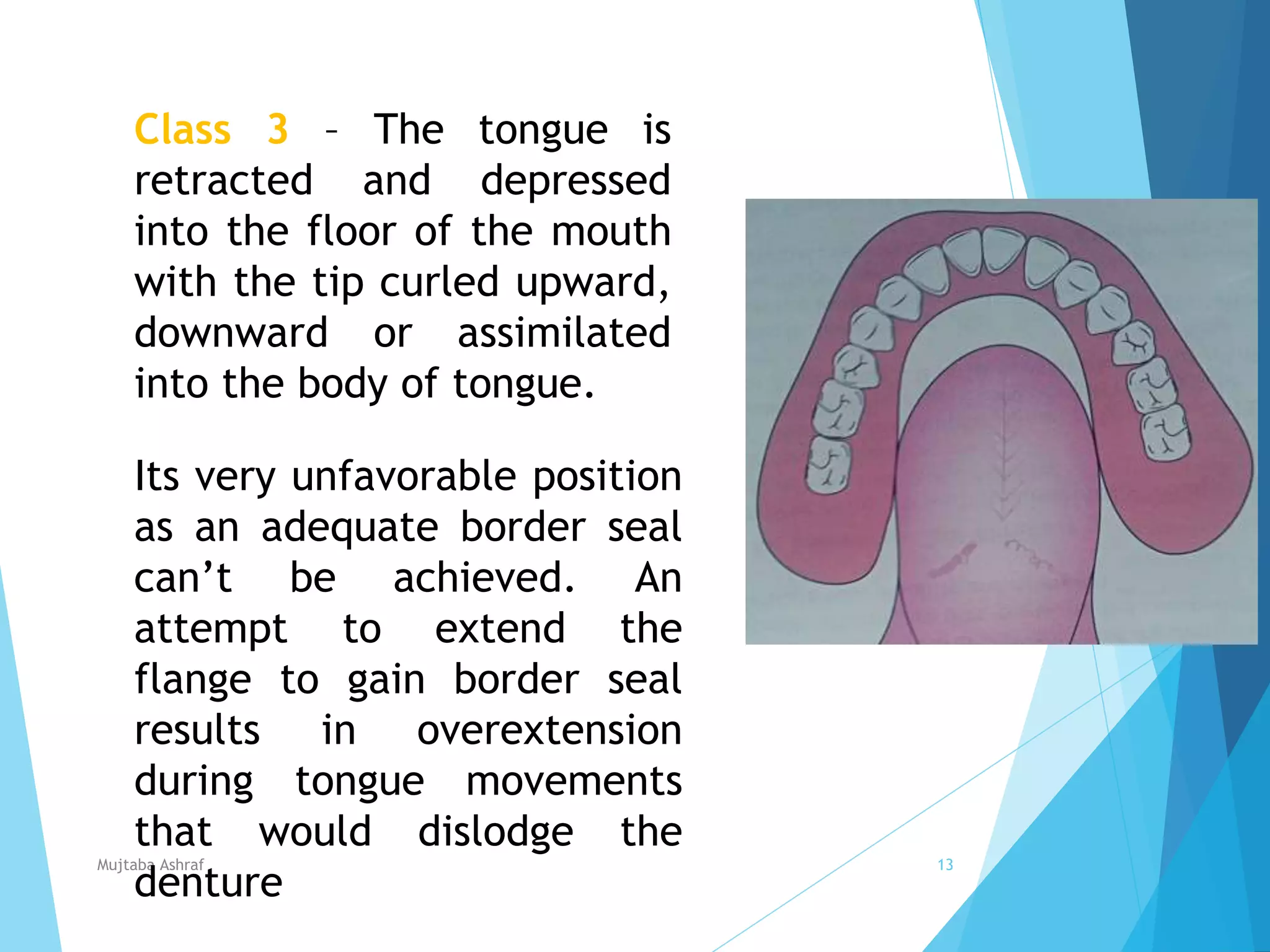
The document discusses the anatomy and function of the tongue. It describes the tongue's structure, muscles, blood supply, nerve supply, papillae, taste buds, development, and functions such as speech and manipulation of food. The tongue is divided into oral and pharyngeal parts and contains intrinsic and extrinsic muscles that protrude, retract, depress, and elevate it. Its main functions are speech, tasting, and assisting with mastication and swallowing of food.