Downloaded 1,120 times
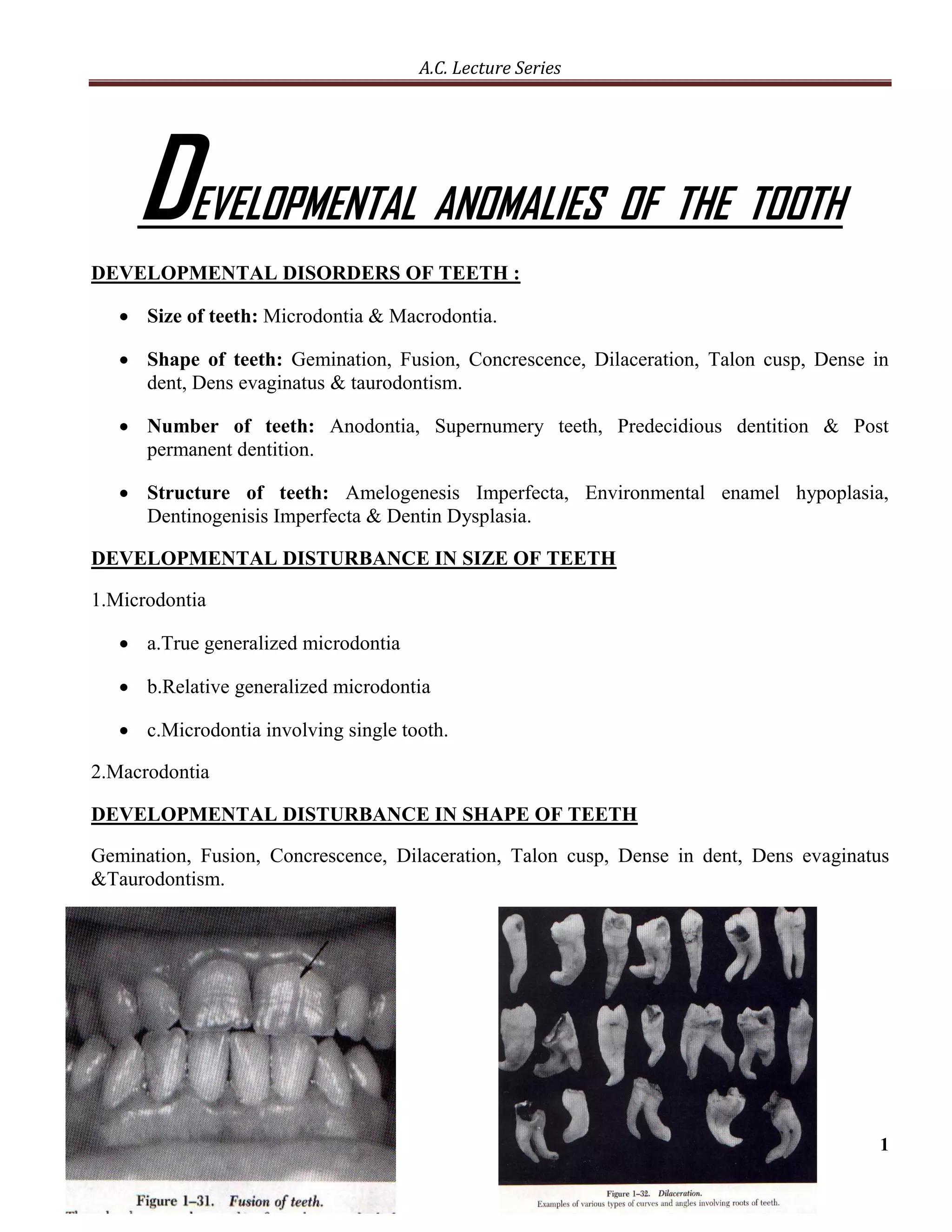














The document discusses various developmental anomalies of teeth, including disturbances in size, shape, number, and structure. It covers conditions like microdontia, macrodontia, gemination, fusion, anodontia, amelogenesis imperfecta, enamel hypoplasia, dentinogenesis imperfecta, and dentin dysplasia. It also discusses agents that can affect tooth development, such as vitamin deficiencies, tetracycline, and fluoride, and how they may incorporate into developing teeth and influence mineralization. Clinical applications regarding how various disturbances can result from disruptions at different stages of tooth development are also mentioned.










































































