
Downloaded 68 times
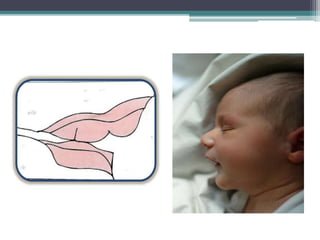
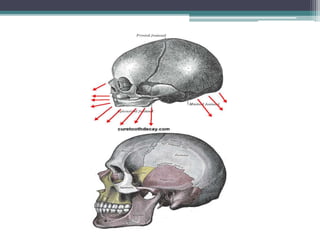
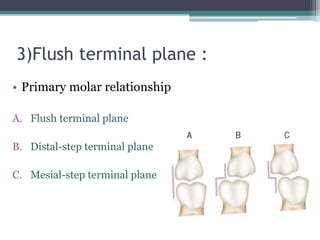
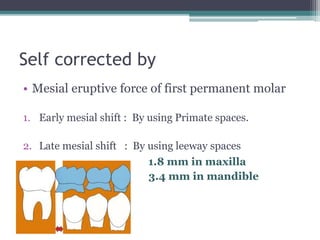



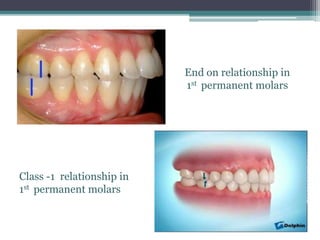
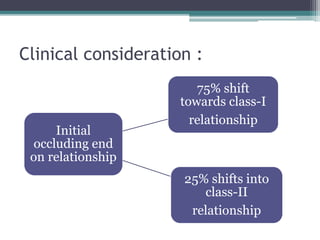
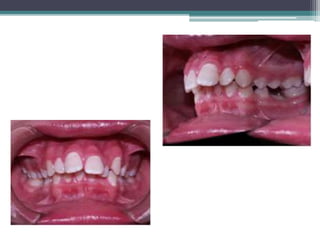
This document discusses self-correcting anomalies that arise during development of the dentition from infancy to adulthood. These anomalies include a retrognathic mandible, anterior open bite, and infantile swallowing in the pre-dental period. In the primary dentition stage, common anomalies are anterior deep bite, spacing, and flush terminal plane. Mixed dentition anomalies include anterior deep bite, mandibular crowding, the ugly duckling stage, and end-on molar relationships. Increased overjet and overbite can occur in the permanent dentition stage. All of these anomalies typically correct themselves without treatment as the jaws and dentition develop through growth and the eruption of permanent teeth.












































































