The Danish study investigates the impact of implantable cardioverter-defibrillator (ICD) therapy on patients with non-ischemic heart failure and reduced ejection fraction receiving contemporary heart failure treatment, including cardiac resynchronization therapy (CRT). Results indicate that while ICDs did not improve overall survival rates, they significantly reduced the risk of sudden cardiac death, particularly in younger patients under 68 years of age. The study underscores the necessity for careful patient selection for ICD implantation due to associated risks and complication rates.
















![Result
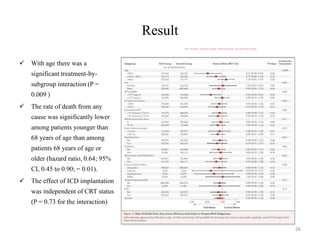
• Primary outcome, death
from any cause, occurred in
120 patients (21.6%) in the
ICD group (4.4 events per
100 person-years) and in
131 patients (23.4%) in the
control group (5.0 events per
100 person-years)
• The hazard ratio for death
from any cause in the ICD
group, as compared with the
control group, was 0.87
(95% confidence interval
[CI] 0.68 to 1.12; P = 0.28)
22
Time-to-Event Curves for Death from Any Cause](https://image.slidesharecdn.com/danishtrial-161220133451/85/DANISH-trial-Cardiology-22-320.jpg)