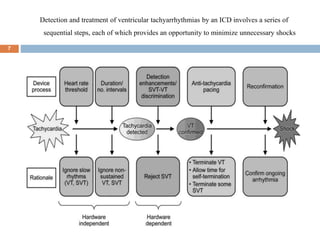
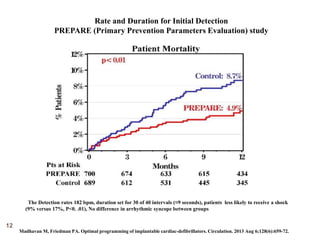
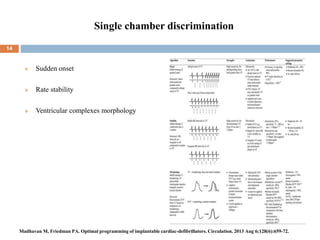
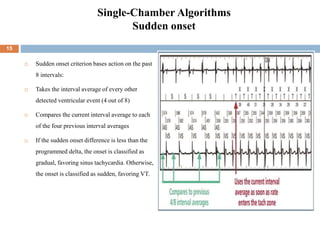
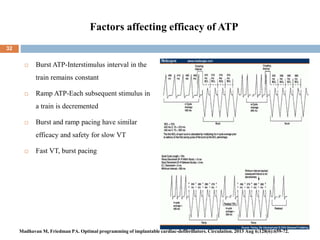
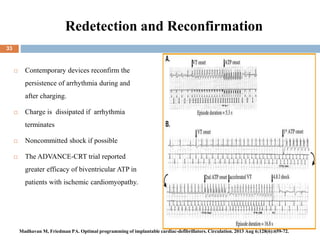
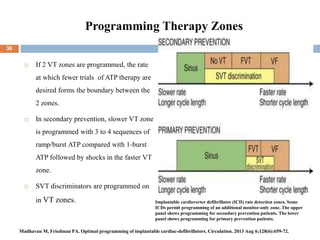
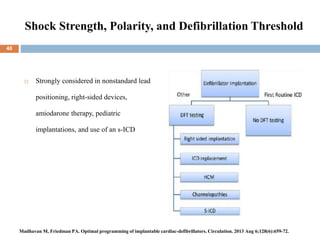
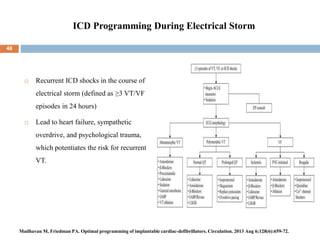
This document summarizes optimal programming of implantable cardiac defibrillators. It discusses sequential steps in detection and treatment of ventricular arrhythmias by ICDs to minimize unnecessary shocks, including programming detection rates and durations, use of antitachycardia pacing, discriminating supraventricular tachycardia from ventricular tachycardia, and programming to minimize noise sensing. It also reviews dual chamber discrimination algorithms and factors affecting efficacy of antitachycardia pacing.