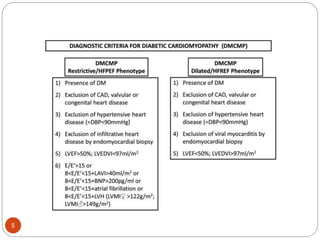
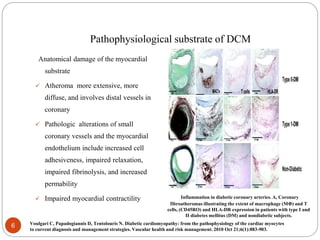
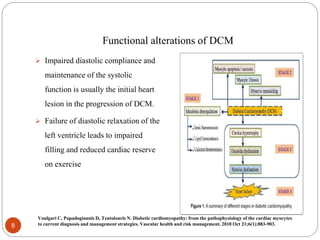
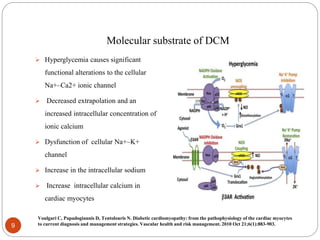
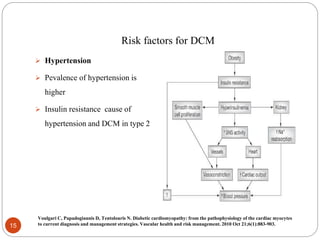
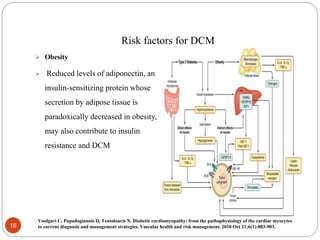
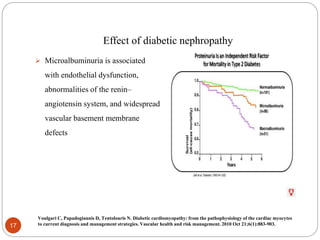
Diabetic cardiomyopathy is characterized by ventricular dysfunction that occurs independently of coronary artery disease or hypertension. Hyperglycemia causes structural and functional damage to cardiac myocytes through increased advanced glycation end products and oxidative stress that impair calcium handling. Other risk factors include insulin resistance, dyslipidemia, hypertension, and obesity. Over time, these factors can lead to myocardial fibrosis and decreased systolic and diastolic function. Strict control of blood sugar and associated cardiovascular risk factors is important to prevent and manage diabetic cardiomyopathy.