Downloaded 57 times


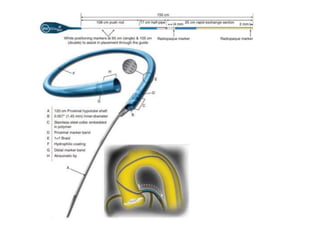
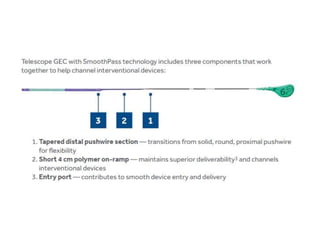

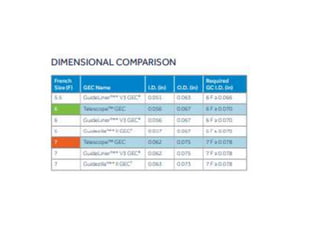

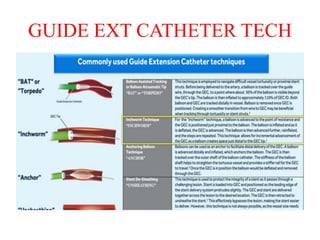
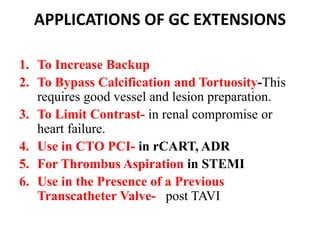


This document discusses guide catheter extensions used in interventional cardiology. It describes four types of guide catheter extensions currently available: Guideliner V2, Guidezilla, Telescope, and Guidion. It provides details on the sizes, lengths, and features of Guideliner V2 and Guidezilla. Applications of guide catheter extensions include increasing backup support, bypassing calcification/tortuosity, limiting contrast use, and facilitating procedures like CTO PCI and thrombus aspiration. Potential complications are discussed, along with tips to minimize risks like dissection or ischemia.





































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

















