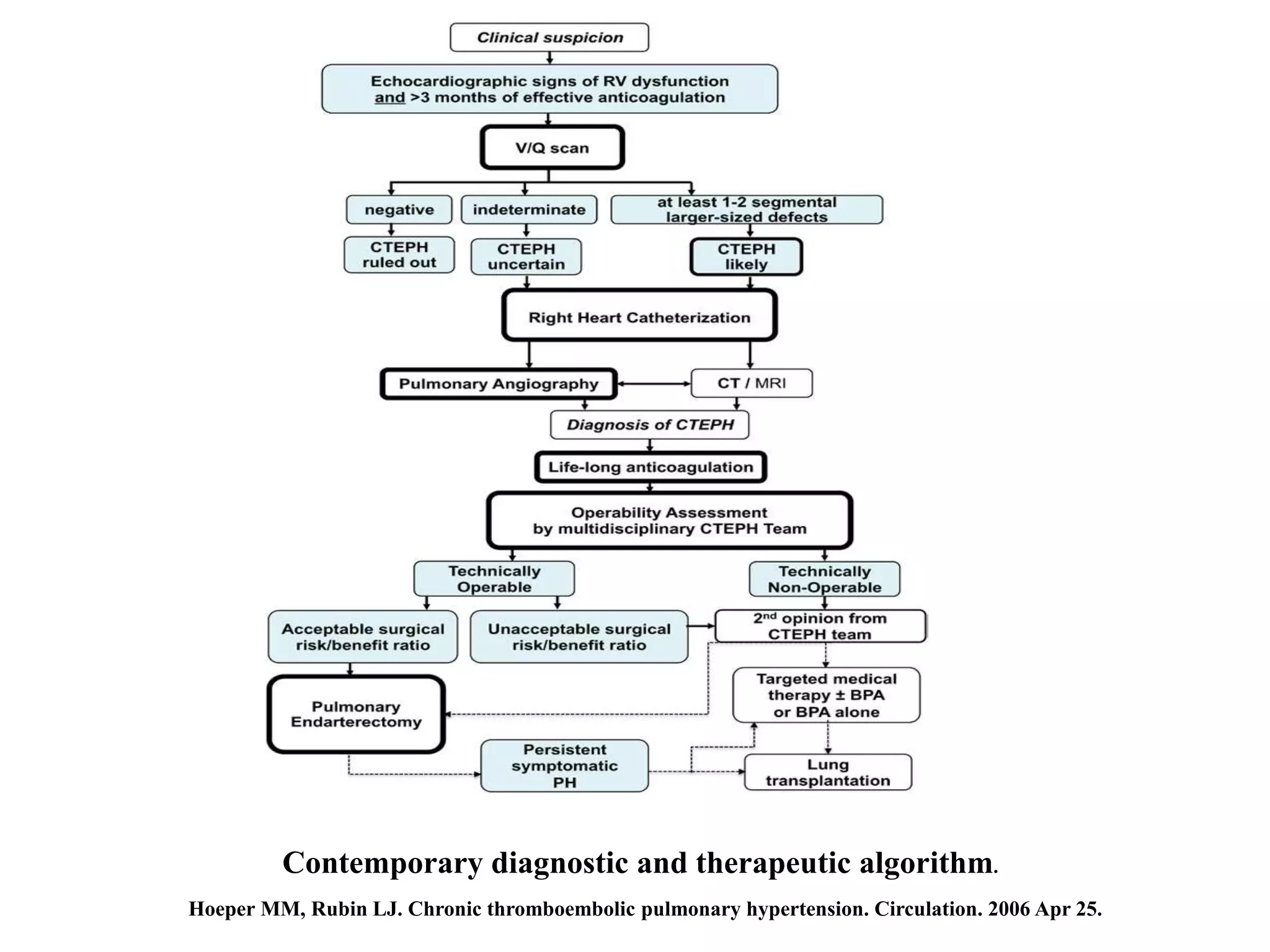
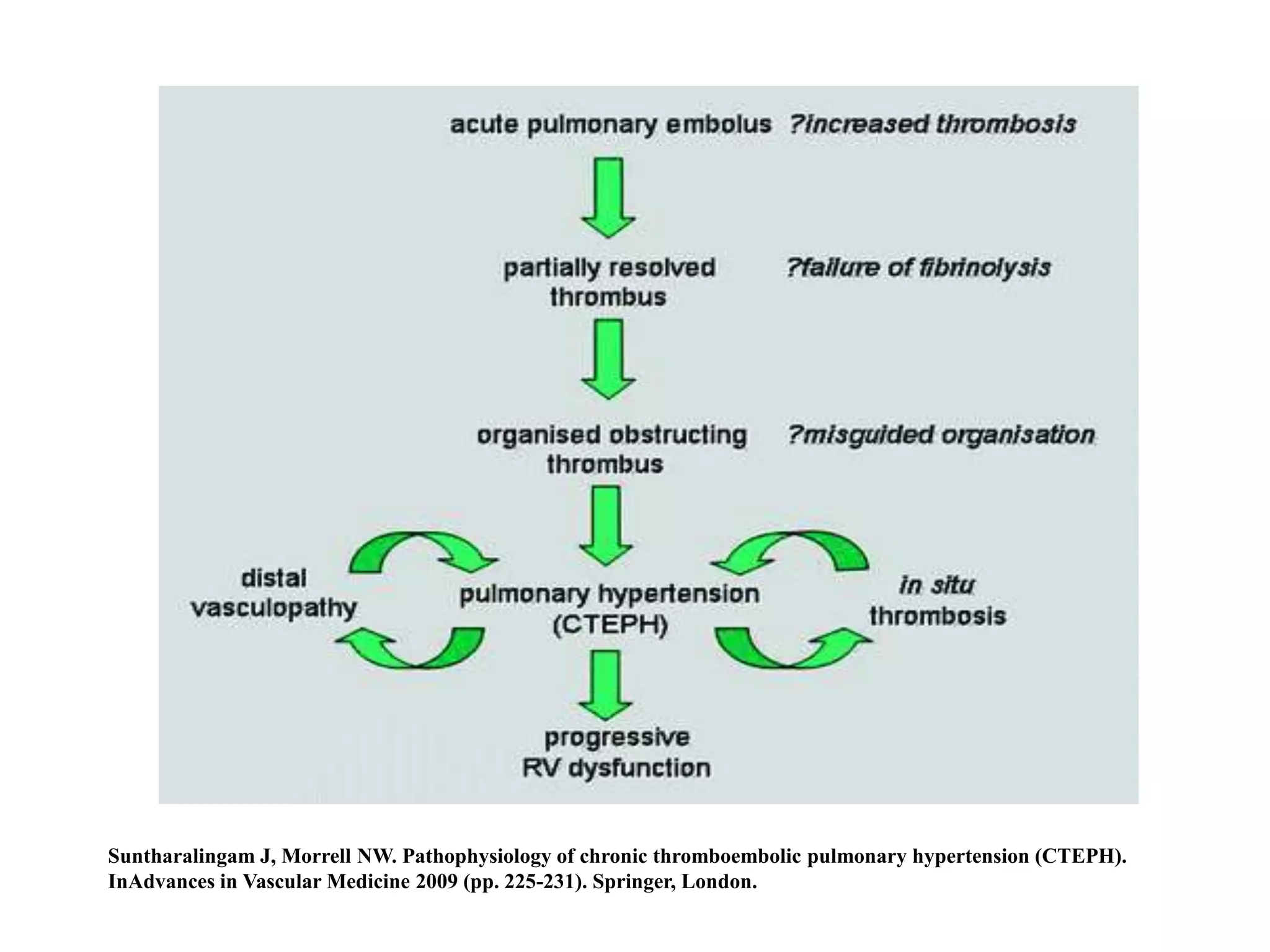
Chronic thromboembolic pulmonary hypertension (CTEPH) is caused by chronic obstruction of the major pulmonary arteries by thrombi. It is amenable to cure by pulmonary endarterectomy (PEA). Diagnosis involves ventilation/perfusion scanning, CT pulmonary angiography, pulmonary angiography, and right heart catheterization to assess pulmonary hypertension. PEA aims to surgically remove the obstructive thrombi and can cure CTEPH if performed at an expert center, where the condition is often underdiagnosed or referred to late.





![Microvasculopathy in chronic thromboembolic pulmonary hypertension involving pulmonary arterioles, venules and capillaries. Schematic representation of
anastomosis between systemic and pulmonary circulation through hypertrophic bronchial arteries and vasa vasorum. PA: pulmonary artery; PVOD: pulmonary
veno-occlusive disease; PAH: pulmonary arterial hypertension. Reproduced and modified from [67] with permission.
Simonneau G, Torbicki A, Dorfmüller P, Kim N. The pathophysiology of chronic thromboembolic pulmonary hypertension. European
Respiratory Review. 2017 Mar 31;26(143):160112.](https://image.slidesharecdn.com/cteph-180731115621/75/Chronic-thromboembolic-pulmonary-hypertension-CTEPH-9-2048.jpg)