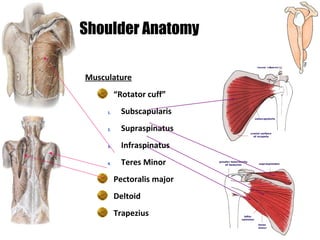
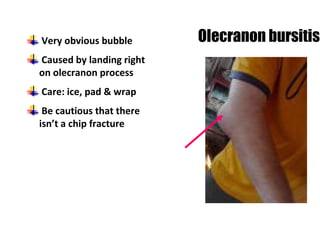
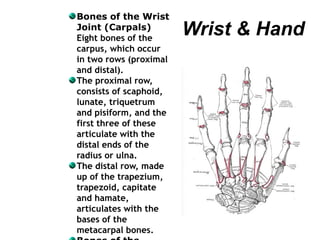
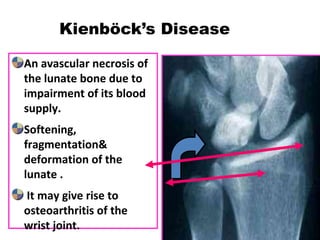
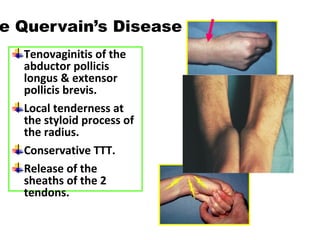
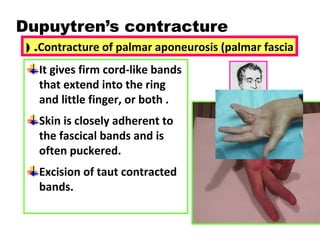
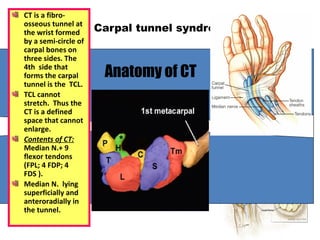
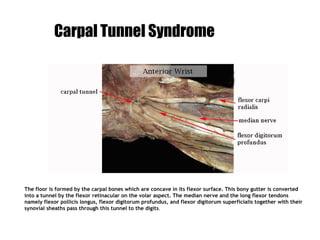
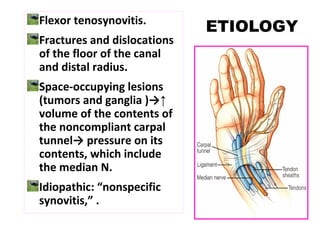
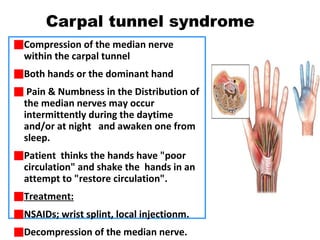
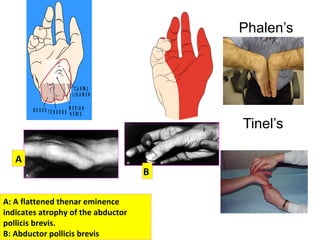
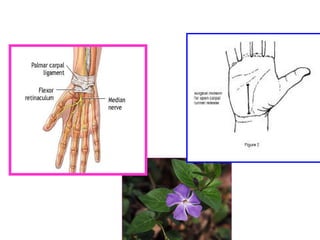
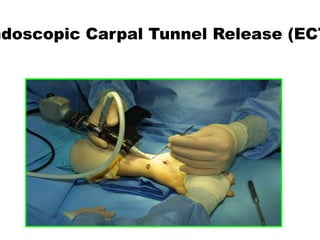
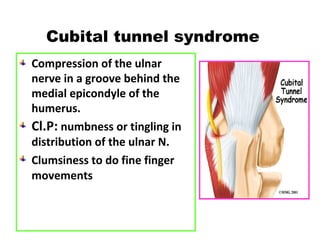
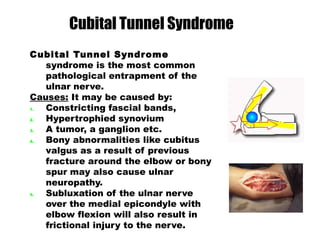
The document discusses disorders of the upper limb, including the shoulder, elbow, wrist, and hand. It provides details on anatomy, common conditions such as frozen shoulder, lateral epicondylitis, carpal tunnel syndrome, and treatments including injections, physical therapy, and surgery. It comprehensively covers the assessment and management of various musculoskeletal issues in the upper extremity.







































































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)











