Downloaded 1,108 times

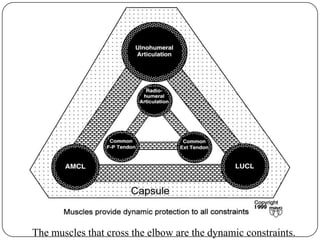









The elbow is stabilized both statically by bony articulations and ligaments, and dynamically by muscles. The three primary static stabilizers are the ulnohumeral articulation, anterior bundle of the MCL, and lateral collateral ligament complex. Muscles that cross the elbow act as dynamic stabilizers. The coronoid process, radial head, and ligaments all play important roles in stability, with the MCL and LCL being the primary soft tissue constraints. Proper biomechanics and force distribution across the elbow joint are necessary for normal function.























































































