The document summarizes the stages of kidney development from the intermediate mesoderm to the metanephros stage. It describes the development of the nephron, collecting system, and vasculature. Key signaling pathways involved include WT1, GDNF-RET, BMP, FGF, PAX-2, and WNT-4. Stages include pronephros regression by 5 weeks, mesonephros functioning until metanephros at 5 weeks, and ascent of kidneys to lumbar region between 6-9 weeks. Applied aspects discussed include anomalies in kidney number, position, ascent, and polycystic kidney disease.
DEVELOPMENT
OF
KIDNEY
- Dr. Garima Aggarwal
- DM Nephrology
- Amrita Institute of Medical Sciences
- Kochi, India Created – September, 2013
2.
OBJECTIVES
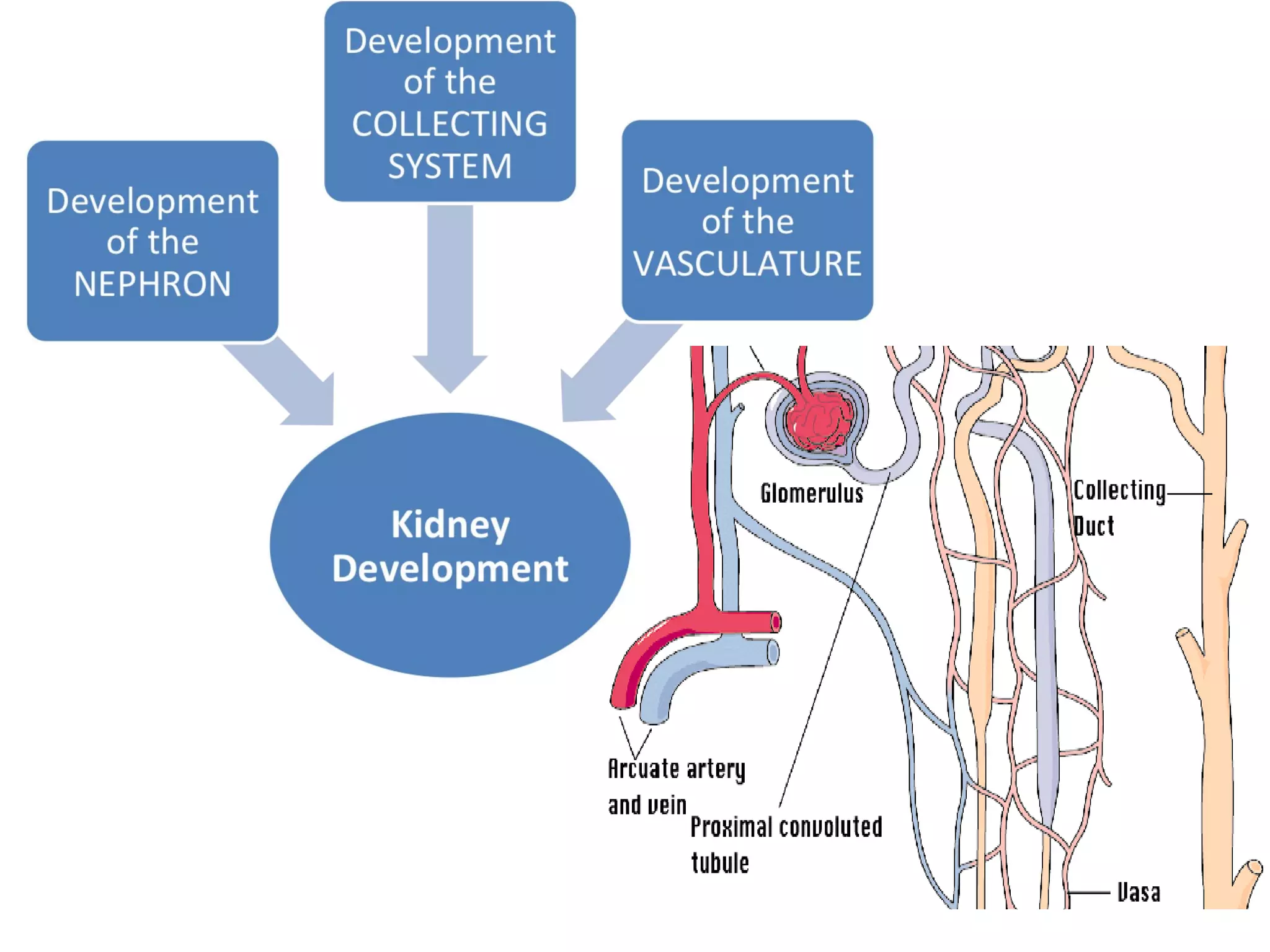
Stages ofKidney Development
Development of Nephron
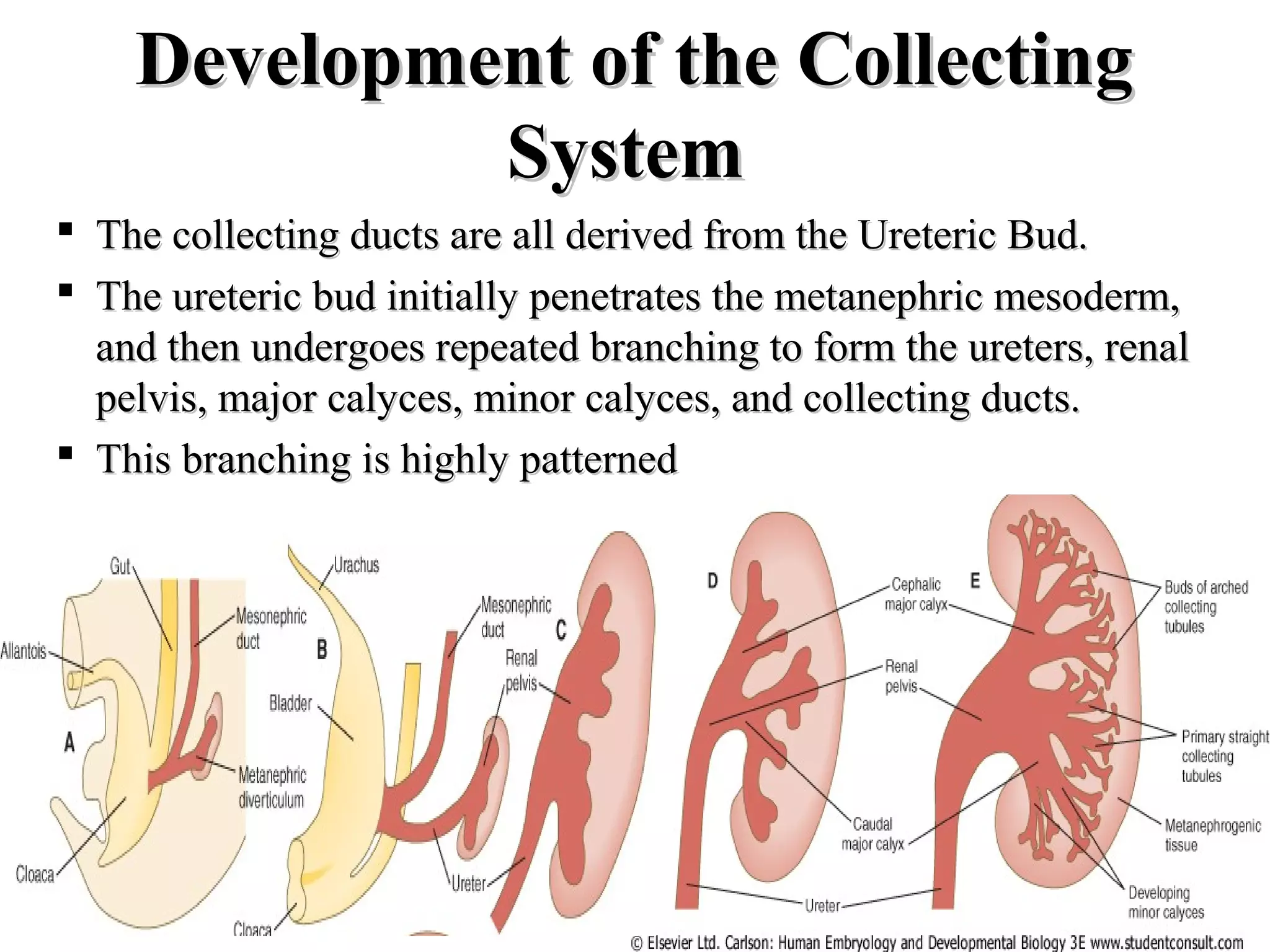
Development of the Collecting System
Development of Vasculature
Molecular Biology
Timeline of Events
Applied Aspects
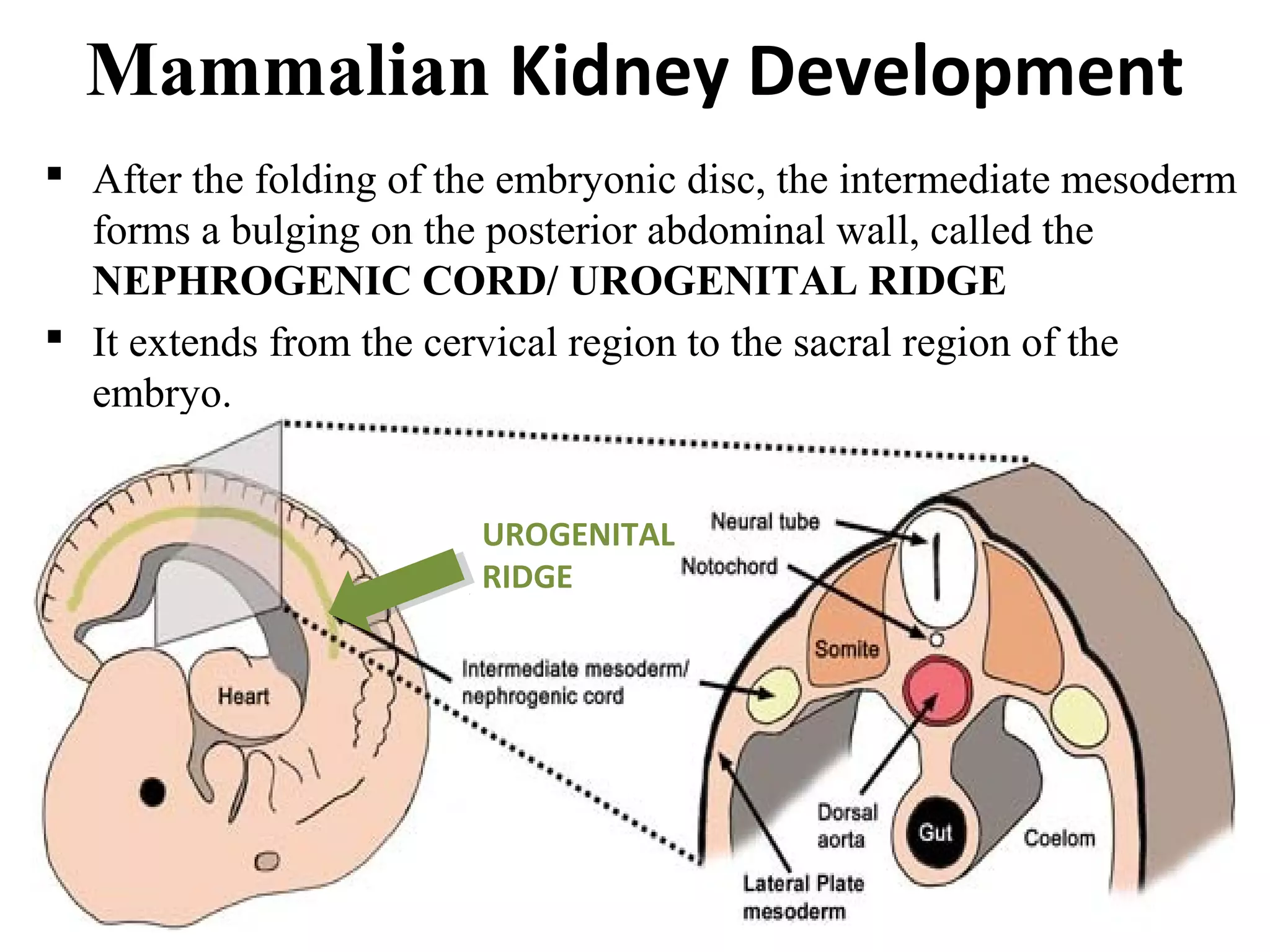
Mammalian Kidney Development
After the folding of the embryonic disc, the intermediate mesoderm
forms a bulging on the posterior abdominal wall, called the
NEPHROGENIC CORD/ UROGENITAL RIDGE
It extends from the cervical region to the sacral region of the
embryo.
UROGENITAL
RIDGE
5.
Stages of KidneyDevelopment
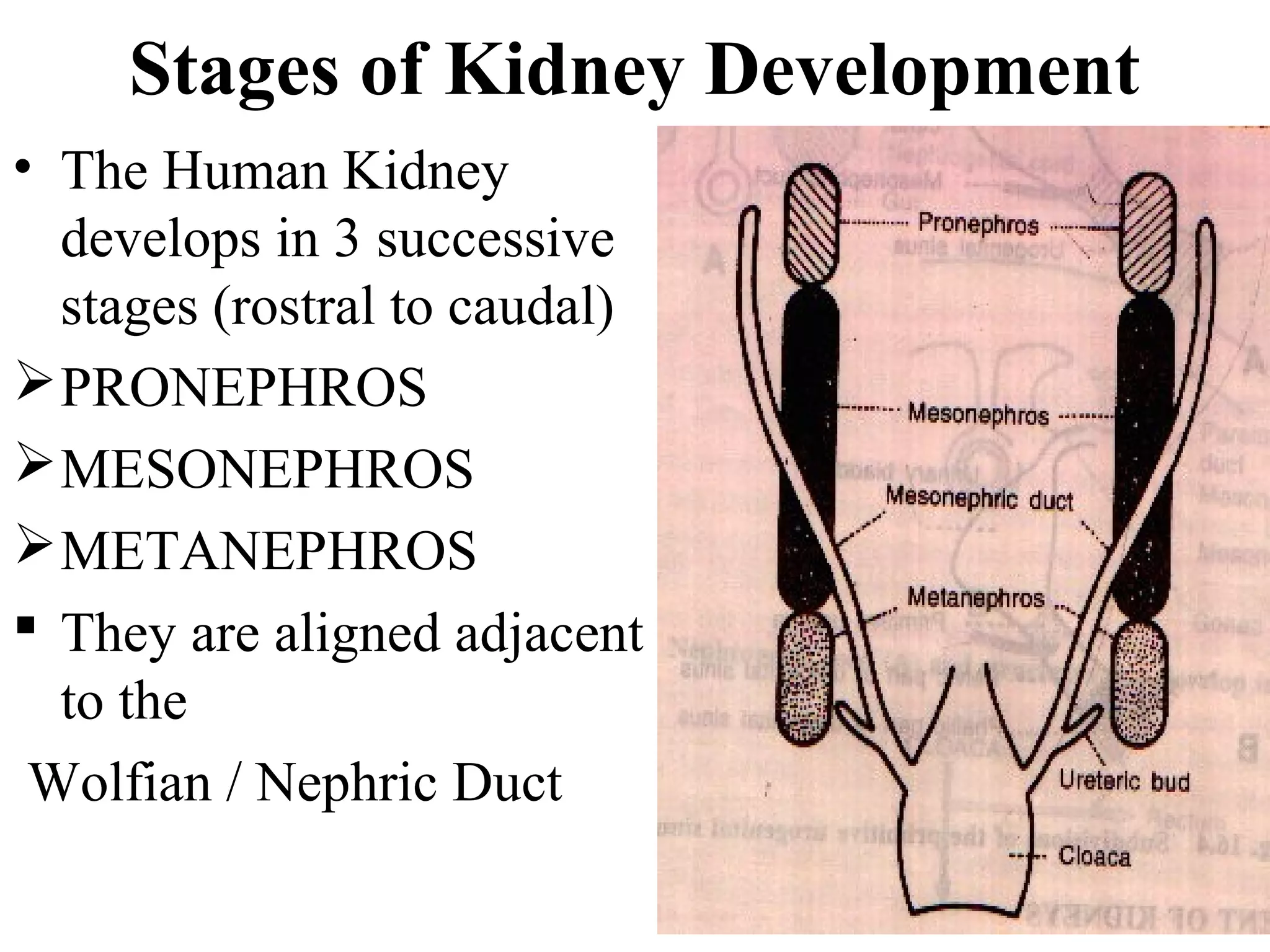
• The Human Kidney
develops in 3 successive
stages (rostral to caudal)
PRONEPHROS
MESONEPHROS
METANEPHROS
They are aligned adjacent
to the
Wolfian / Nephric Duct
MMeessoonneepphhrrooss
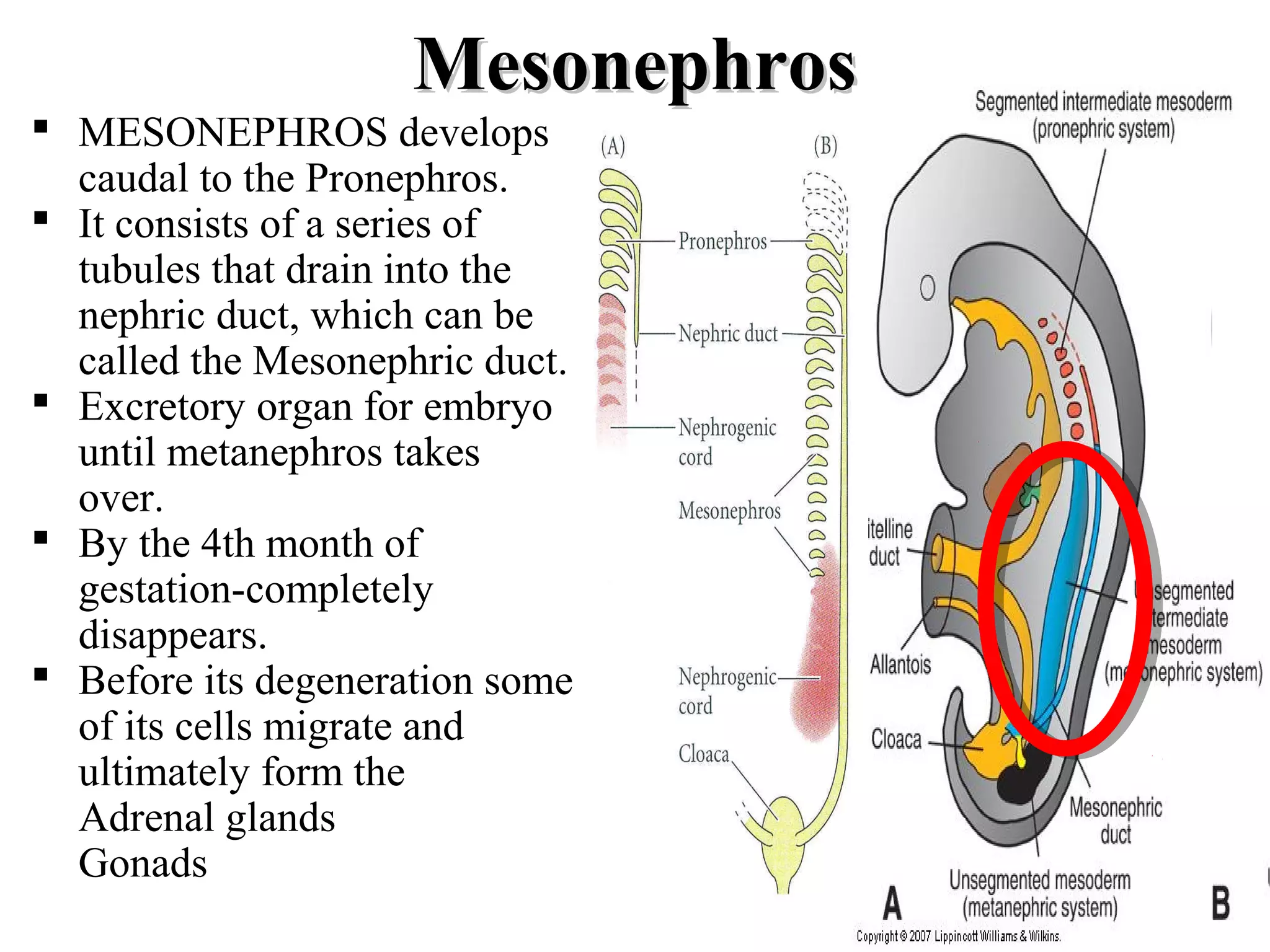
MESONEPHROSdevelops
caudal to the Pronephros.
It consists of a series of
tubules that drain into the
nephric duct, which can be
called the Mesonephric duct.
Excretory organ for embryo
until metanephros takes
over.
By the 4th month of
gestation-completely
disappears.
Before its degeneration some
of its cells migrate and
ultimately form the
Adrenal glands
Gonads
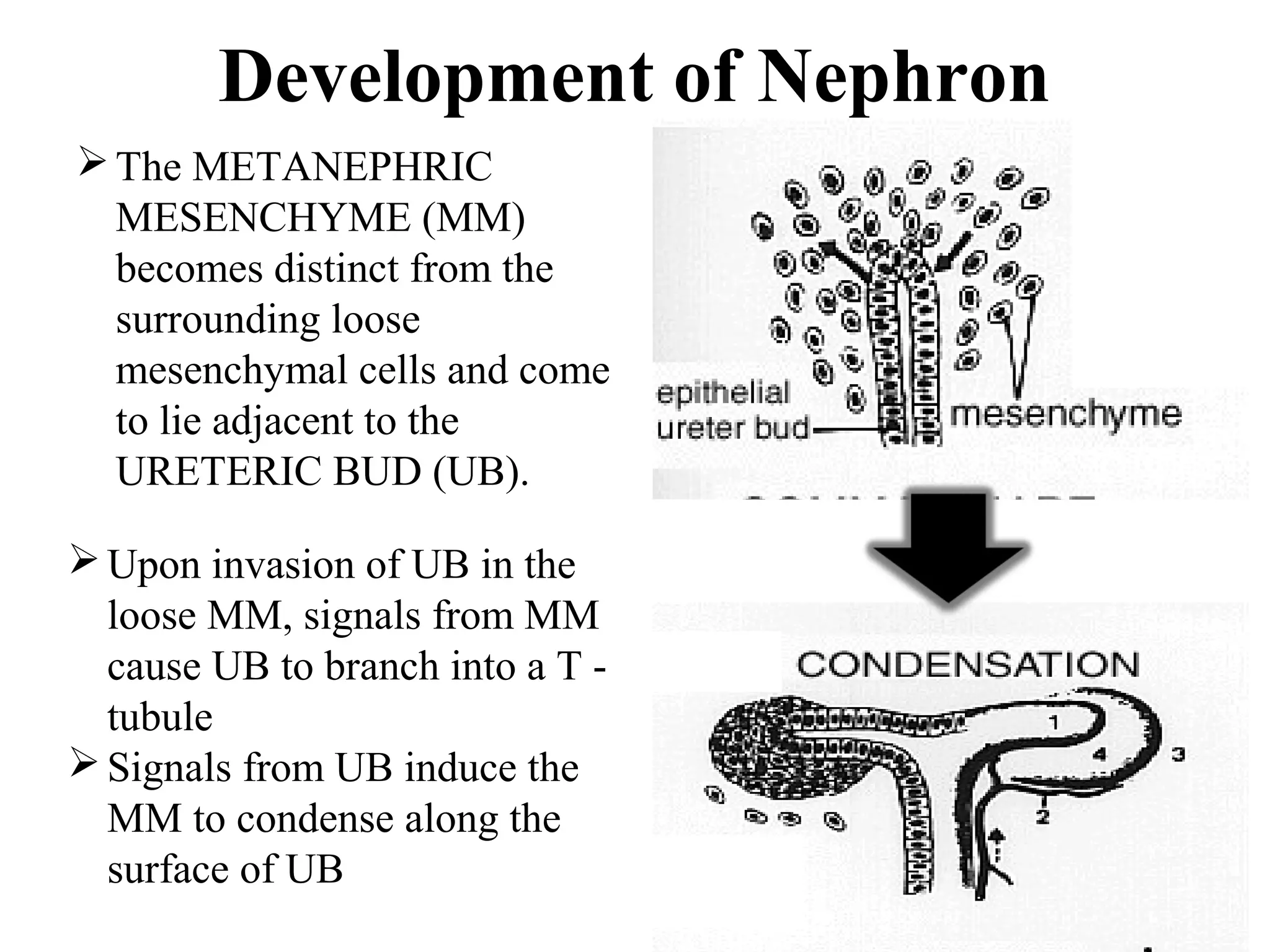
Development of Nephron
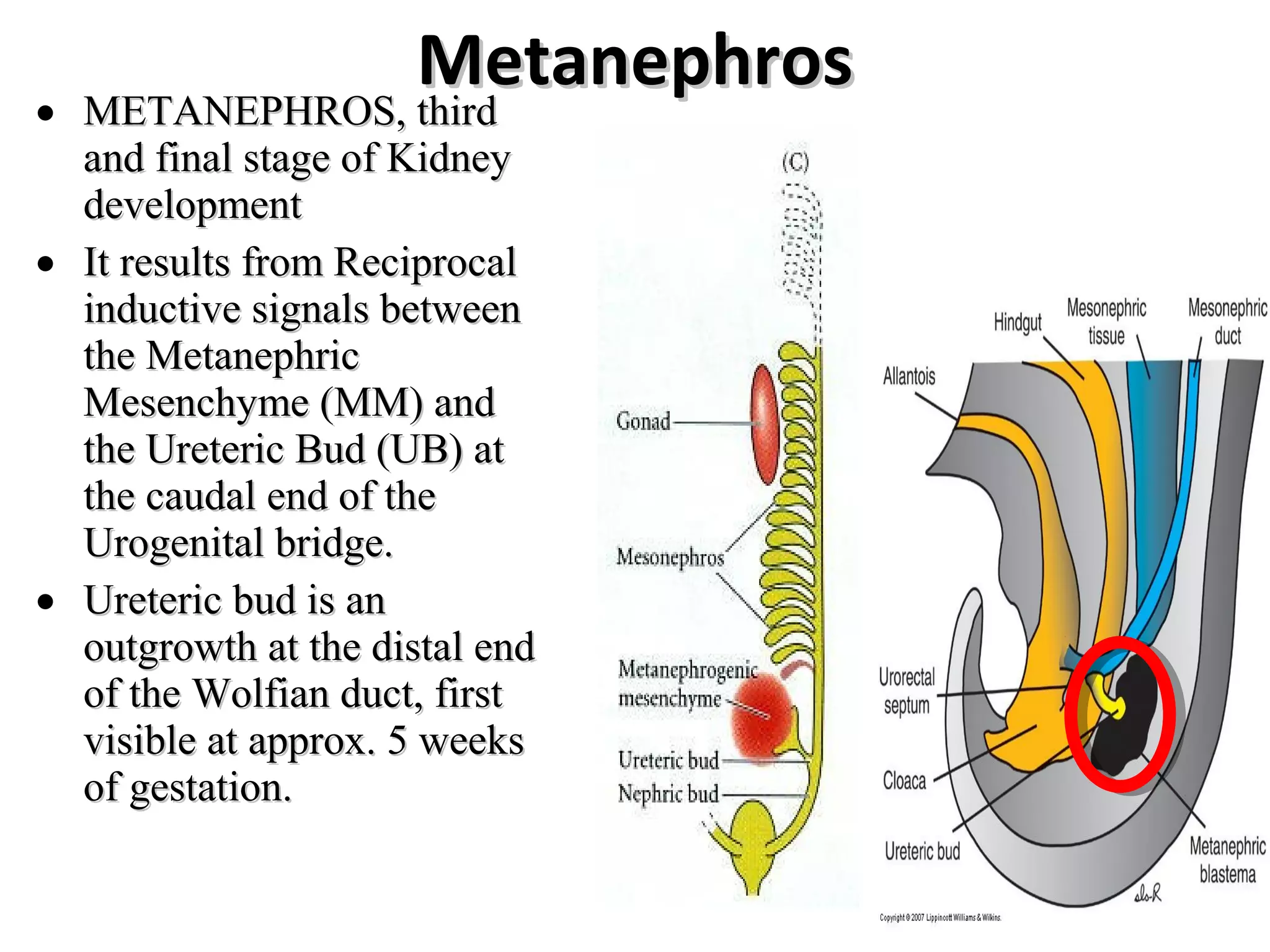
The METANEPHRIC
MESENCHYME (MM)
becomes distinct from the
surrounding loose
mesenchymal cells and come
to lie adjacent to the
URETERIC BUD (UB).
Upon invasion of UB in the
loose MM, signals from MM
cause UB to branch into a T -
tubule
Signals from UB induce the
MM to condense along the
surface of UB
11.
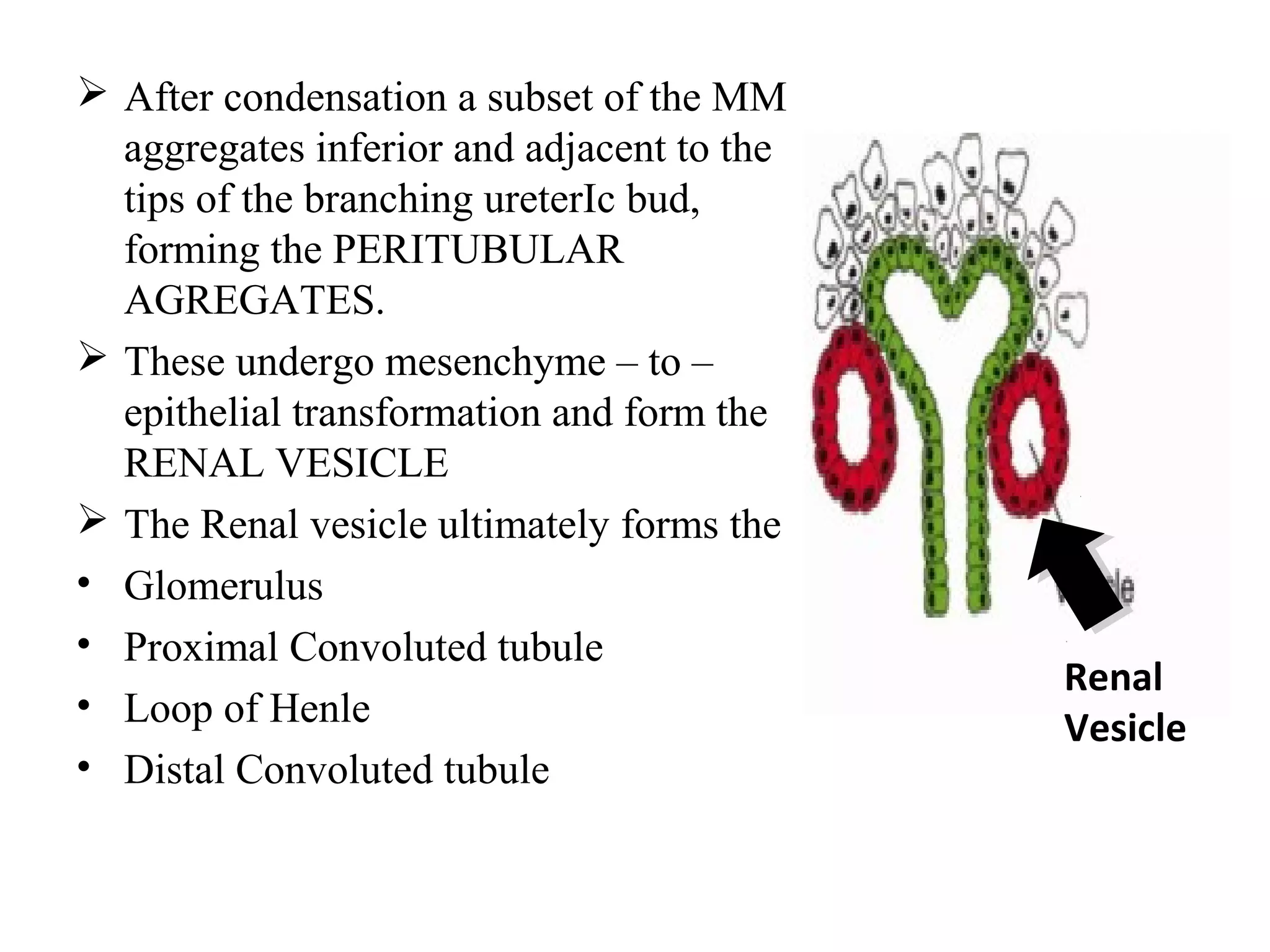
After condensationa subset of the MM
aggregates inferior and adjacent to the
tips of the branching ureterIc bud,
forming the PERITUBULAR
AGREGATES.
These undergo mesenchyme – to –
epithelial transformation and form the
RENAL VESICLE
The Renal vesicle ultimately forms the
• Glomerulus
• Proximal Convoluted tubule
• Loop of Henle
• Distal Convoluted tubule
Renal
Vesicle
12.
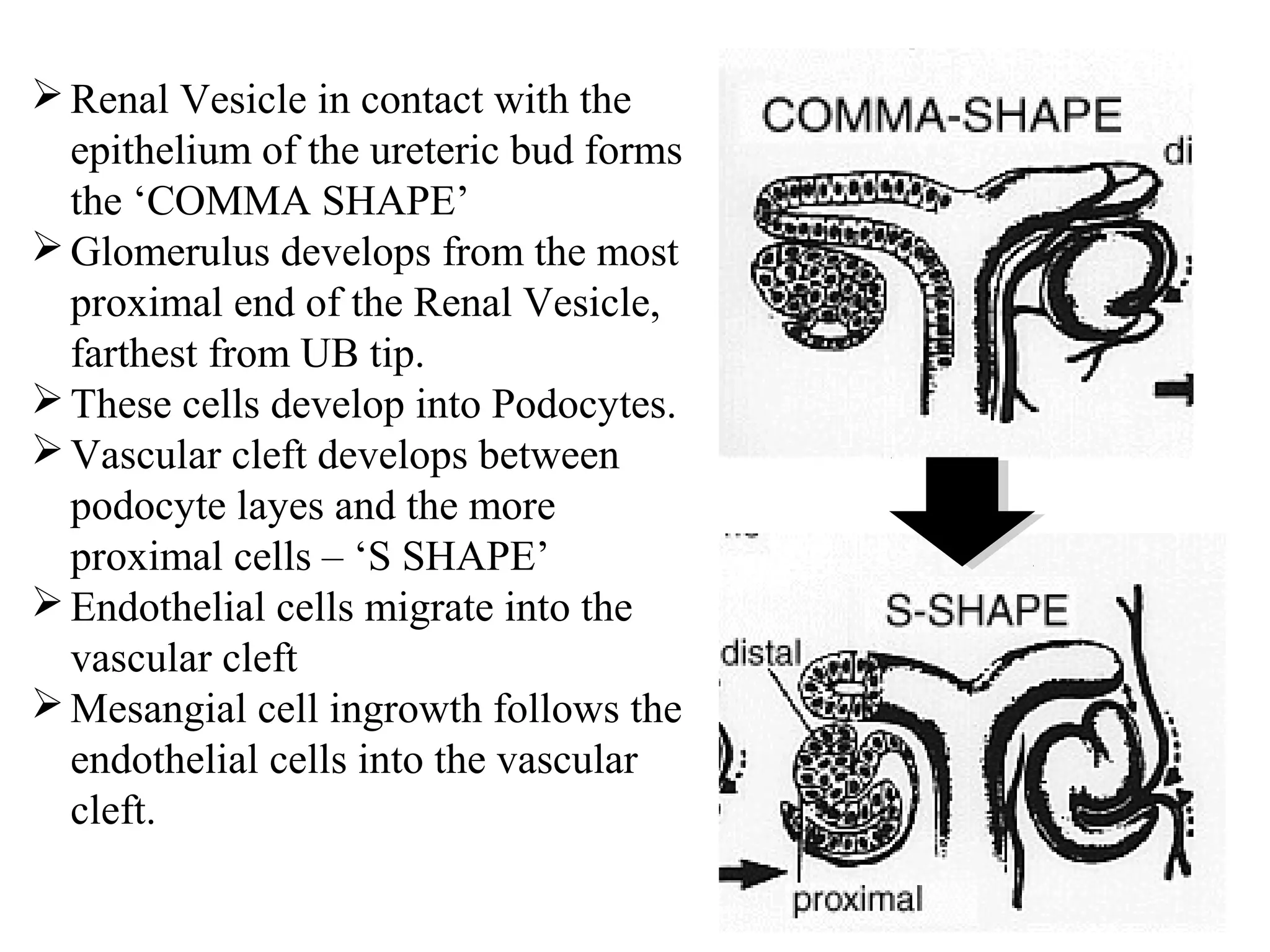
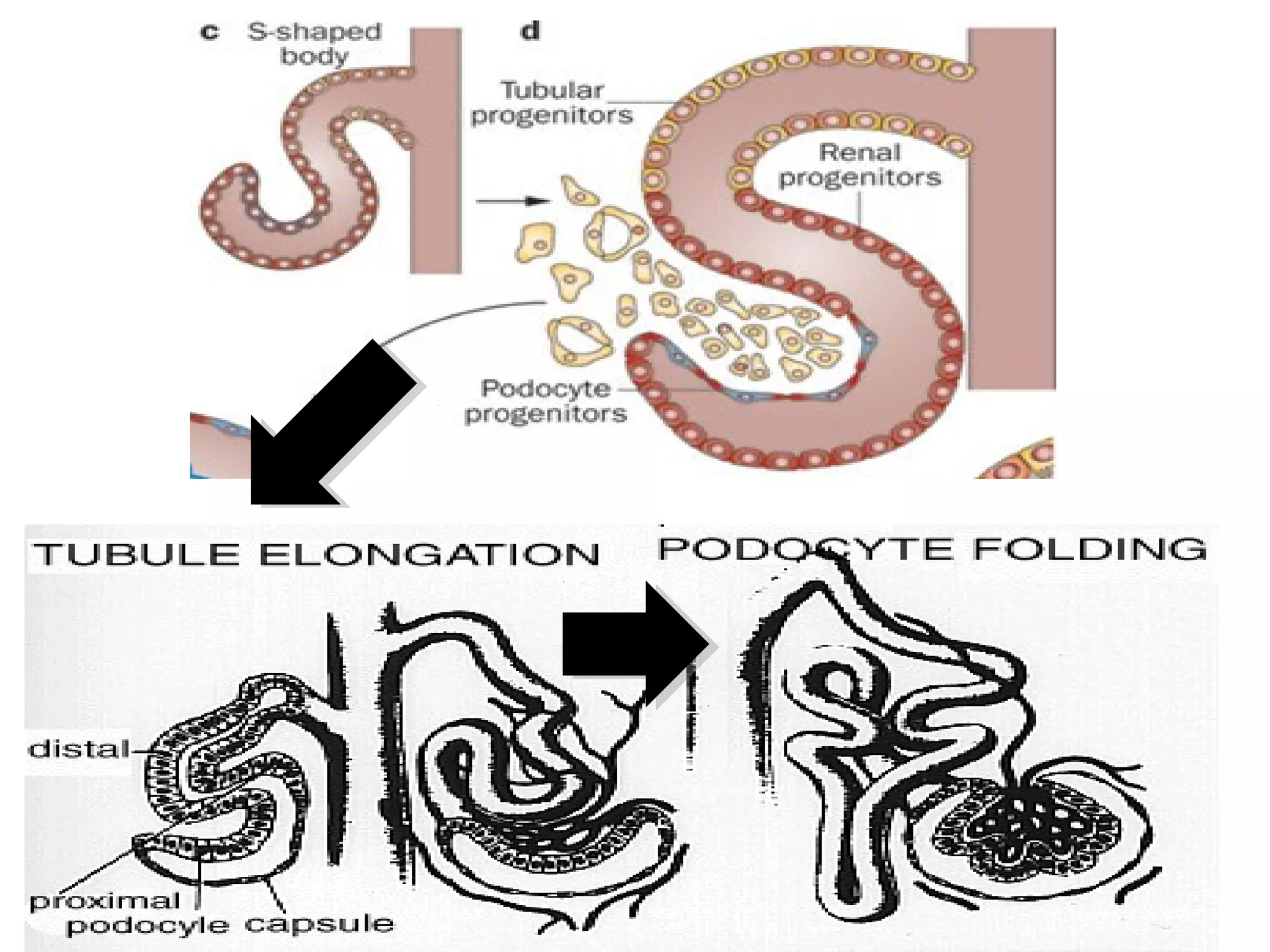
Renal Vesicle incontact with the
epithelium of the ureteric bud forms
the ‘COMMA SHAPE’
Glomerulus develops from the most
proximal end of the Renal Vesicle,
farthest from UB tip.
These cells develop into Podocytes.
Vascular cleft develops between
podocyte layes and the more
proximal cells – ‘S SHAPE’
Endothelial cells migrate into the
vascular cleft
Mesangial cell ingrowth follows the
endothelial cells into the vascular
cleft.
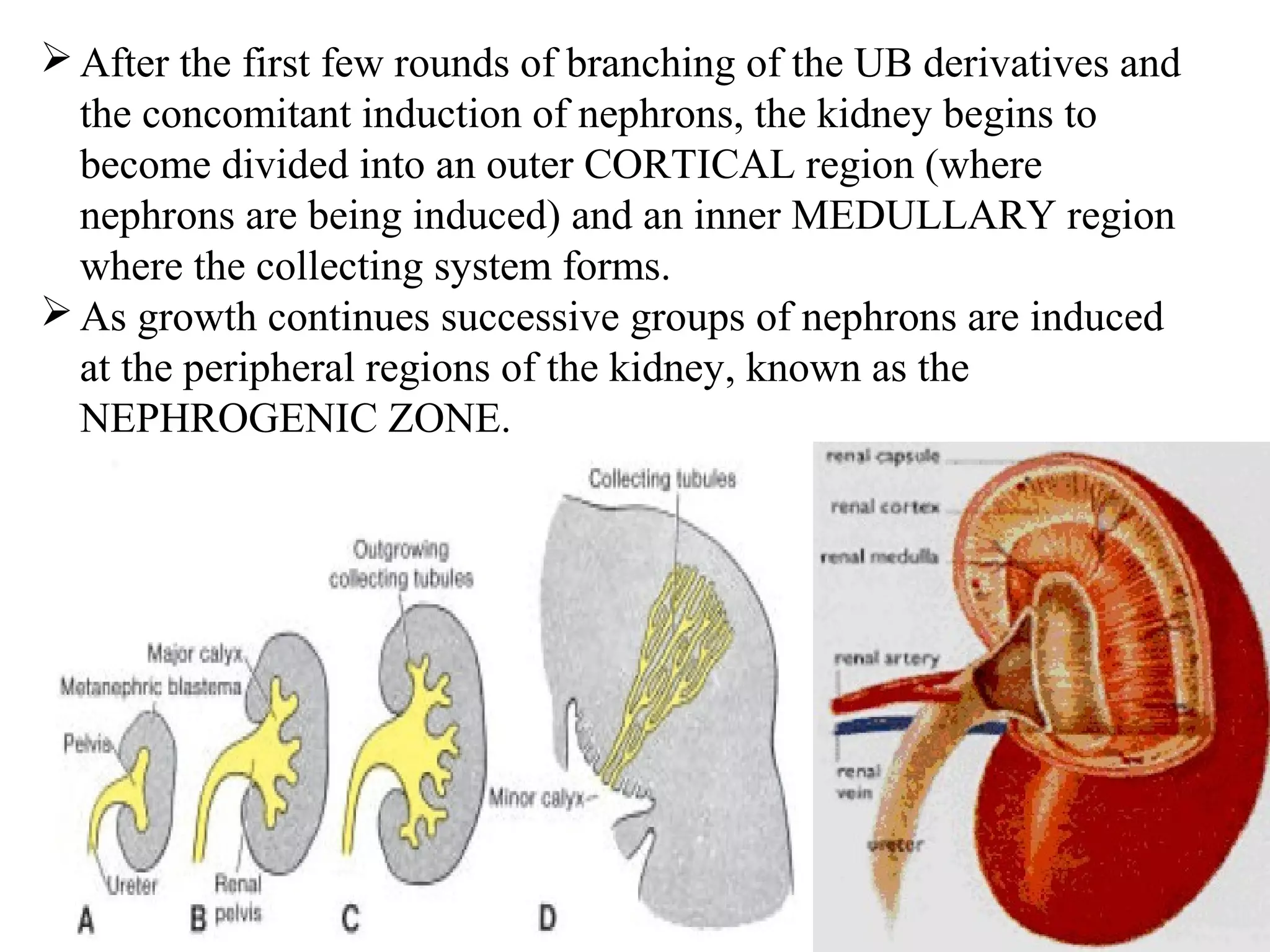
After the firstfew rounds of branching of the UB derivatives and
the concomitant induction of nephrons, the kidney begins to
become divided into an outer CORTICAL region (where
nephrons are being induced) and an inner MEDULLARY region
where the collecting system forms.
As growth continues successive groups of nephrons are induced
at the peripheral regions of the kidney, known as the
NEPHROGENIC ZONE.
16.
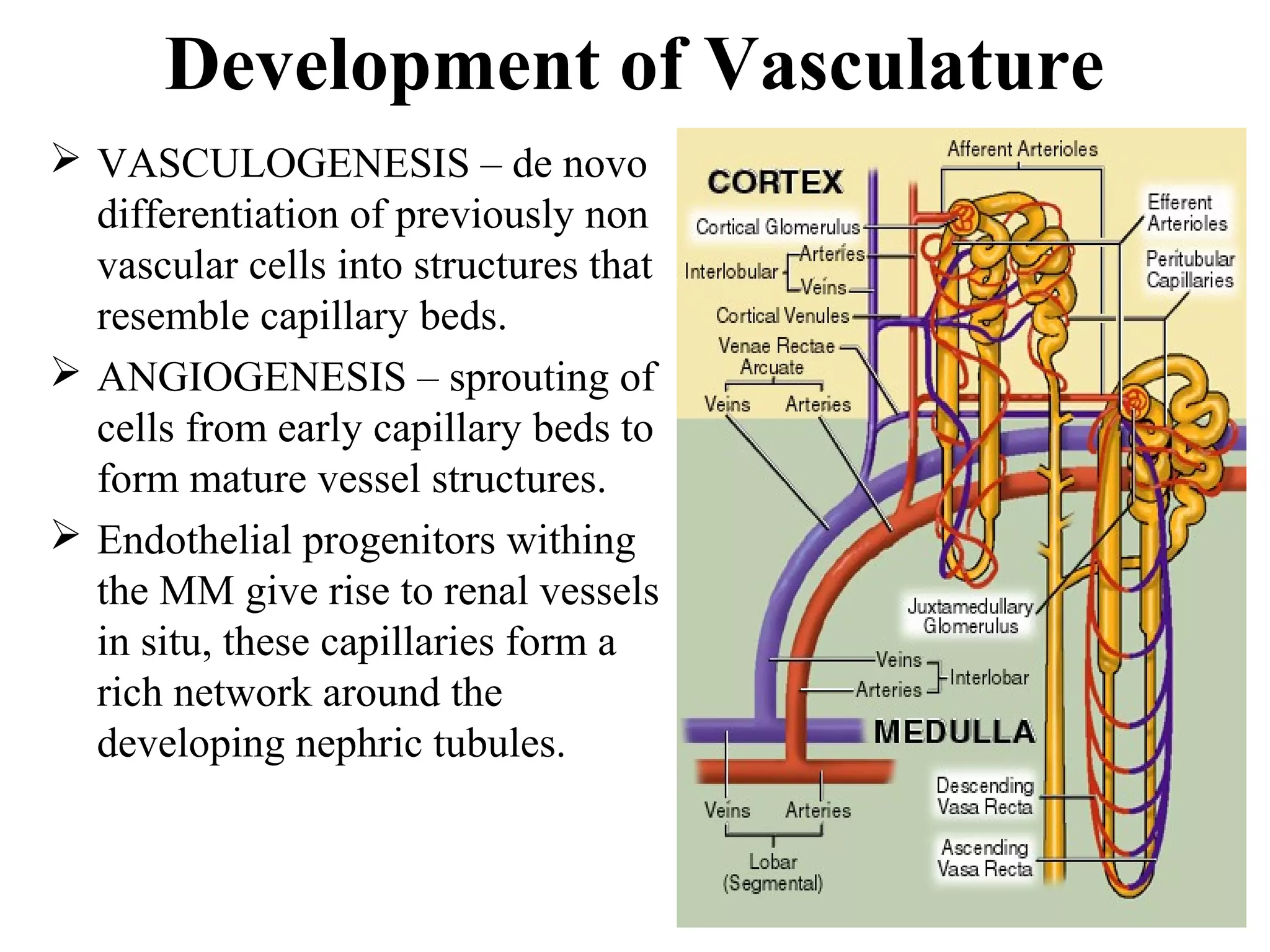
Development of Vasculature
VASCULOGENESIS – de novo
differentiation of previously non
vascular cells into structures that
resemble capillary beds.
ANGIOGENESIS – sprouting of
cells from early capillary beds to
form mature vessel structures.
Endothelial progenitors withing
the MM give rise to renal vessels
in situ, these capillaries form a
rich network around the
developing nephric tubules.
17.
Renal Ascent
a The fetal metanephros is located att vveerrtteebbrraall lleevveell SS11--SS22,,
wwhheerreeaass tthhee ddeeffiinniittiivvee aadduulltt kkiiddnneeyy iiss llooccaatteedd aatt vveerrtteebbrraall lleevveell
TT1122--LL33..
From 6th to 9th weeks: kidneys ascend to a lumbar site just
below adrenals
As the kidneys migrate, they are vascularized by a succession of
transient aortic sprouts that arise at progressively higher levels
final pair forms in the upper lumbar region and becomes the
definitive renal arteries
occasionally, a more inferior pair of arteries persists as accessory
lower pole arteries
IInniittiiaallllyy tthhee kkiiddnneeyyss ffaaccee aanntteerriioorrllyy,, bbuutt dduurriinngg tthhee aasscceenntt,, tthhee
kkiiddnneeyyss rroottaattee 9900°°ccaauussiinngg tthhee hhiilluumm ttoo ffiinnaallllyy ffaaccee mmeeddiiaallllyy..
18.
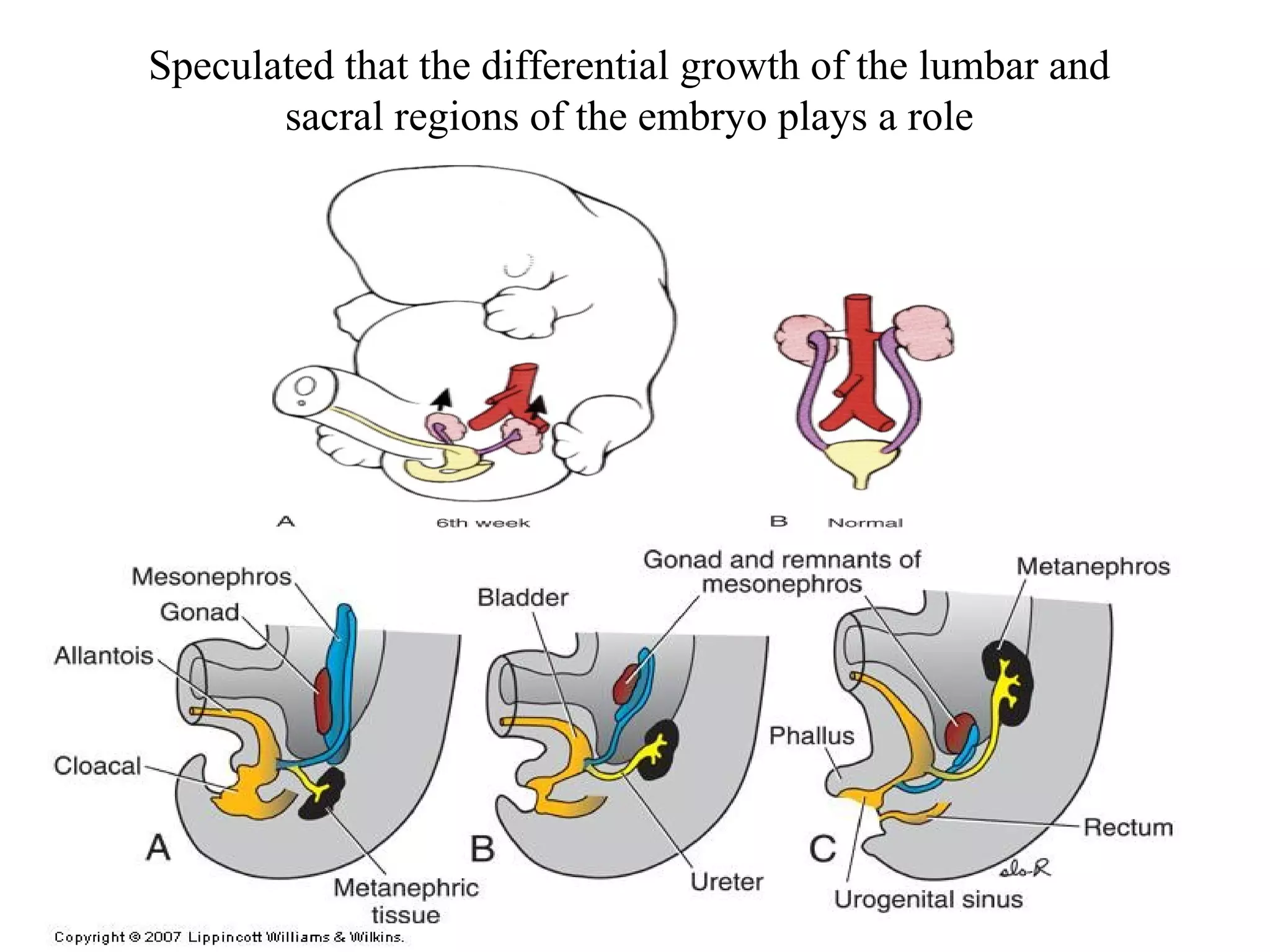
Speculated that thedifferential growth of the lumbar and
sacral regions of the embryo plays a role
19.
Signaling Pathways inKidney
Development
• From MM
– WT 1
• Hepatocyte Growth Factor(HGF) & MET
• Glial derived nuerotrophic factor(GDNF) & RET
• From Ureteric bud
• Bone morphogenic protein(BMP)
• Fibroblast growth factor(FGF)
• PAX-2
• WNT-4
20.
WT1
• Wt1is a transcription factor
• WT1 was originally identified as a gene involved in Wilms tumor, a pediatric cancer in
which kidney elements are incompletely differentiated and proliferate to form
tumors.
• Wt1 is first expressed in intermediate mesoderm prior to kidney development, and
then in the kidney, gonads and mesothelium.
• Makes MM tissue to respond to ureteric bud induction.
21.
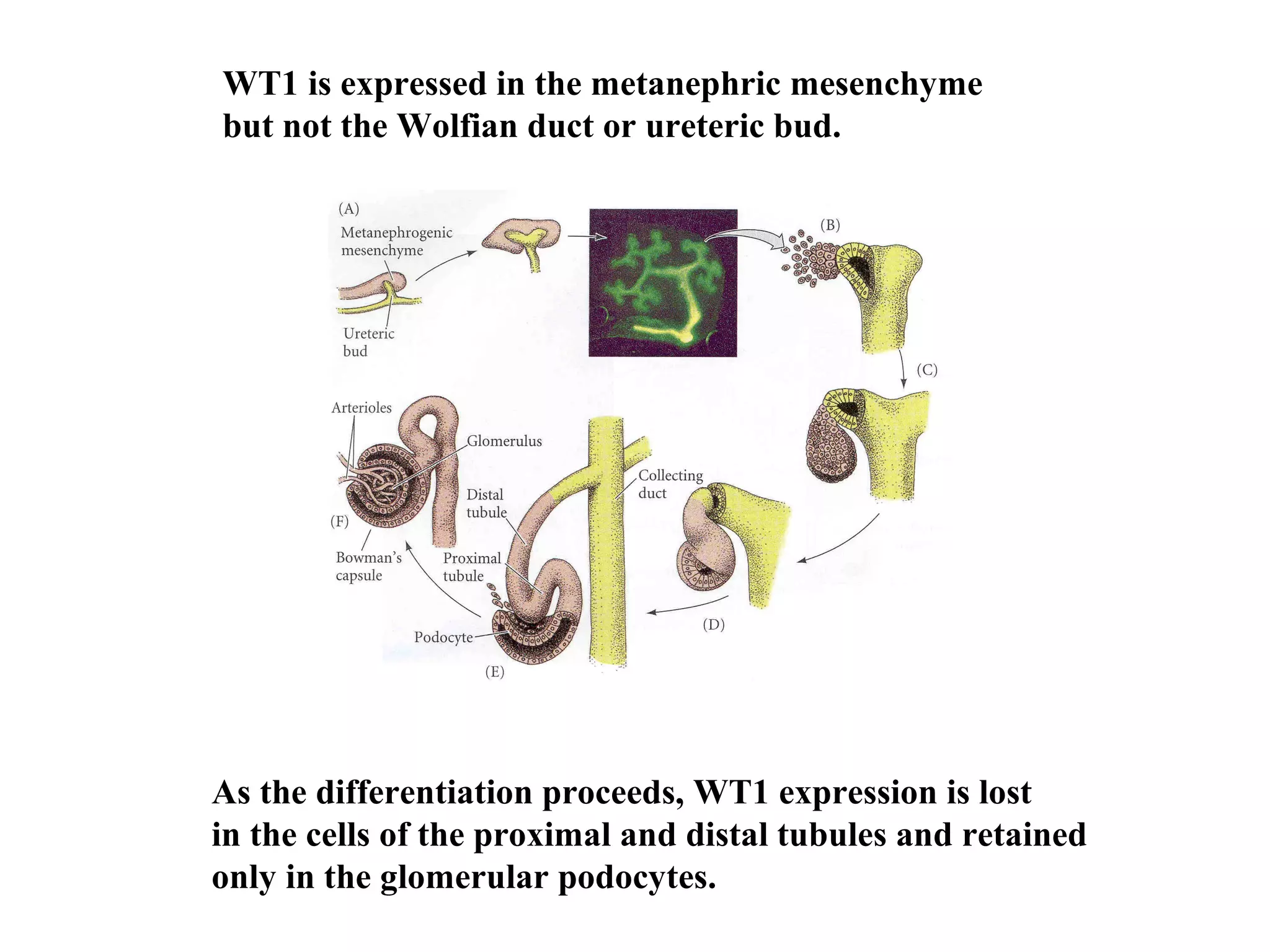
WT1 is expressedin the metanephric mesenchyme
but not the Wolfian duct or ureteric bud.
As the differentiation proceeds, WT1 expression is lost
in the cells of the proximal and distal tubules and retained
only in the glomerular podocytes.
22.
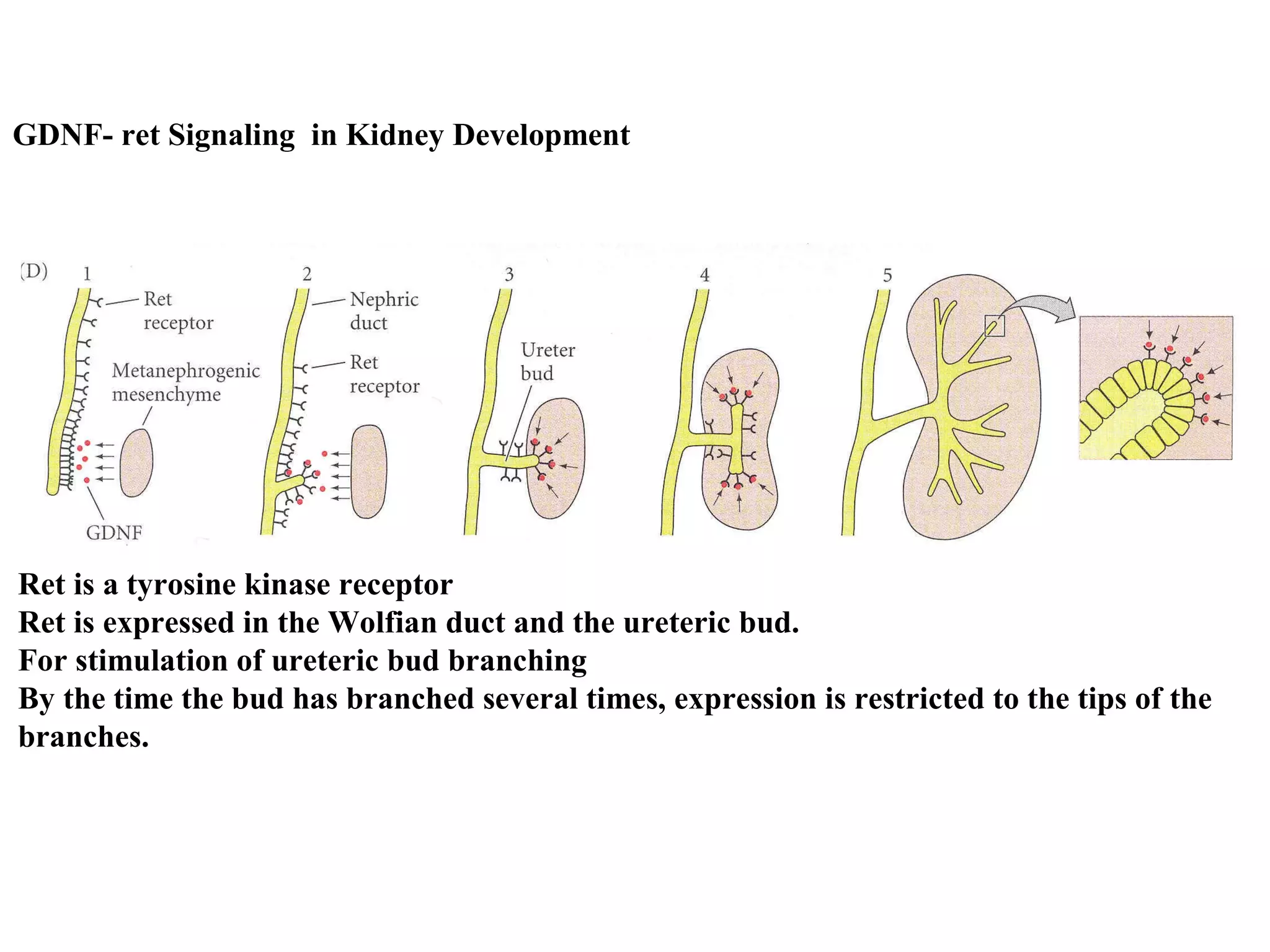
GDNF- ret Signalingin Kidney Development
Ret is a tyrosine kinase receptor
Ret is expressed in the Wolfian duct and the ureteric bud.
For stimulation of ureteric bud branching
By the time the bud has branched several times, expression is restricted to the tips of the
branches.
23.
Factors from UreteralBud
• Bone morphogenic protein(BMP)
• Fibroblast growth factor(FGF)
- Stimulate proliferation of metanephric mesenchyme
- Maintain production of WT 1.
24.
Factors from UreteralBud
• PAX-2
• WNT-4
- Mainly cause mesenchyme to epithelialise in
prepation for excretory tubule differentiation.
- Production of Laminin and Type 4 Collagen to
form basement membrane.
25.
Timeline of KidneyEmbryology
• Week 4 : appearance of Wolffian or
Mesonephric Duct
• Day 28 : formation of Ureteric Bud (UB)
• Week 4-8 : Initial MM induction and UB
branching
• Week 8 : First nephrons are formed
• Week 6-8 : kidneys ascend from pelvis to
lumbar location
• Week 8-15 : Period of UB branching with
stochastic formation of UB ampulla and nephron units
• Week 10 : filtration begins
• Week 32-36: End of Nephrogenesis
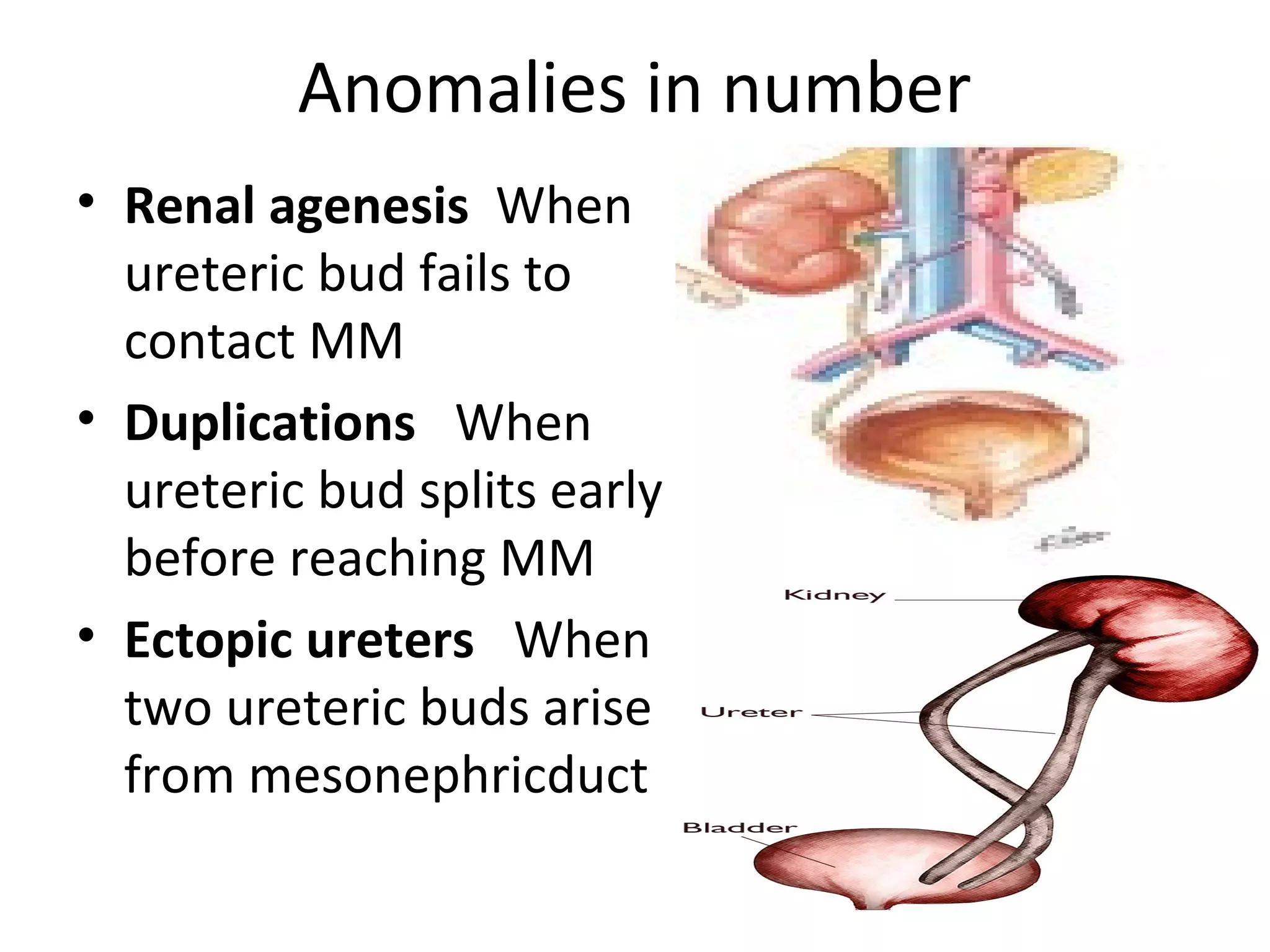
Anomalies in number
• Renal agenesis When
ureteric bud fails to
contact MM
• Duplications When
ureteric bud splits early
before reaching MM
• Ectopic ureters When
two ureteric buds arise
from mesonephricduct
28.
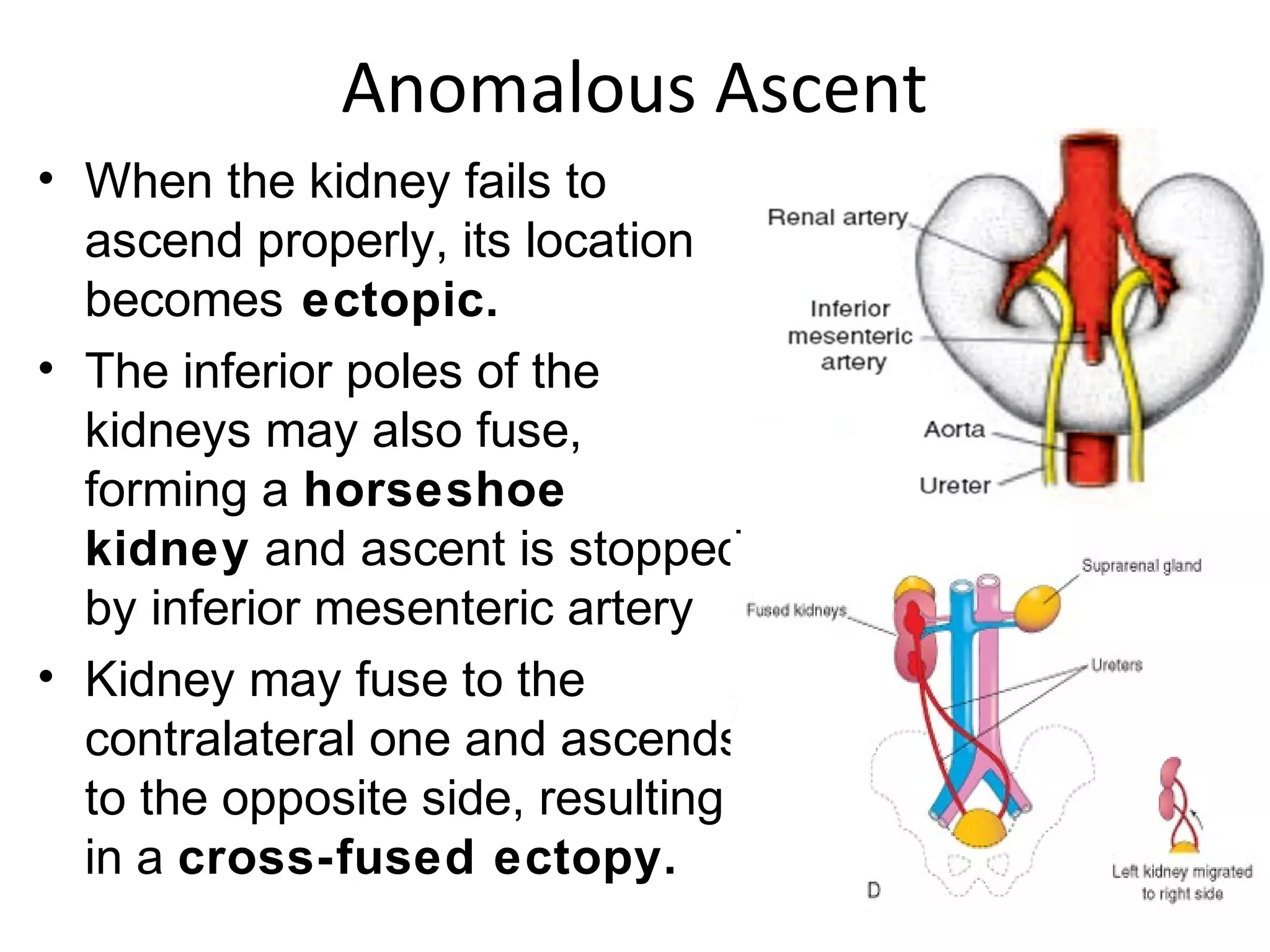
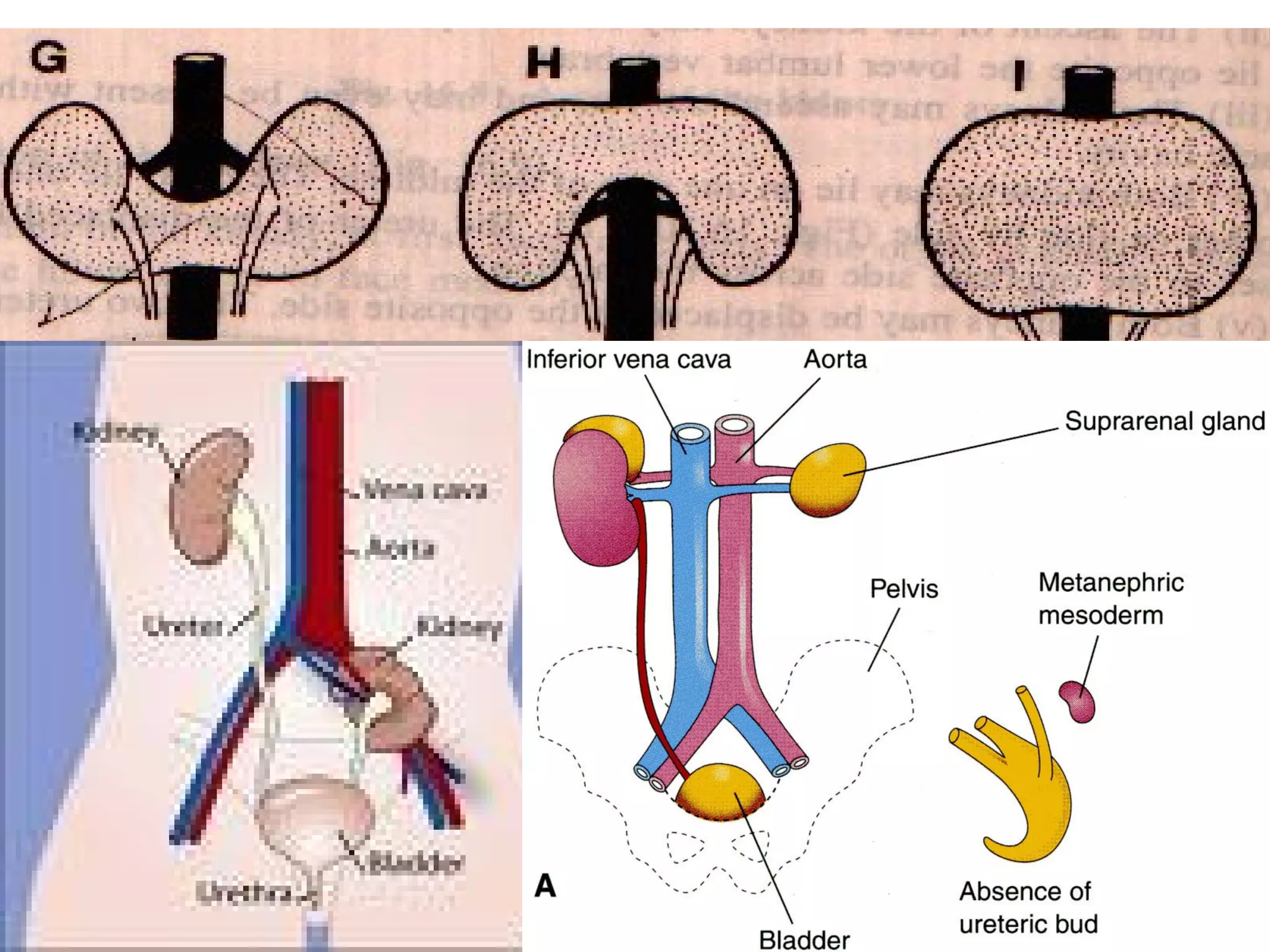
Anomalous Ascent
•When the kidney fails to
ascend properly, its location
becomes ectopic.
• The inferior poles of the
kidneys may also fuse,
forming a horseshoe
kidney and ascent is stopped
by inferior mesenteric artery
• Kidney may fuse to the
contralateral one and ascends
to the opposite side, resulting
in a cross-fused ectopy.
30.
Anomalous position
•Malrotated Kidneys - Calyces face
anteriorly or antrolaterally. Have
some element of obstruction
causing inadequate drainage –
leading to infection & stone
formation
Other abnormal positions include-
• Ventral Position
• Ventromedial Position
• Dorsal Position
• Lateral Position
31.
Mal rotated kidneys
• Calyces face anteriorly or
antrolaterally
• Have some element of
obstruction causing
inadequate drainage –
leading to infection & stone
formation
30-march, 2010, tuesday 31
32.
Polycystic kidneys
•Hereditary – autosomal dominant
• Not manifested before 30
• Kidneys enlarged, studded with cysts
• Unyeilding capsule compresses renal
parenchyma causing atrophy
• Liver,lungs and pancreas may be affected
• Defact : not clear, many theories
30-march, 2010, tuesday 32
33.
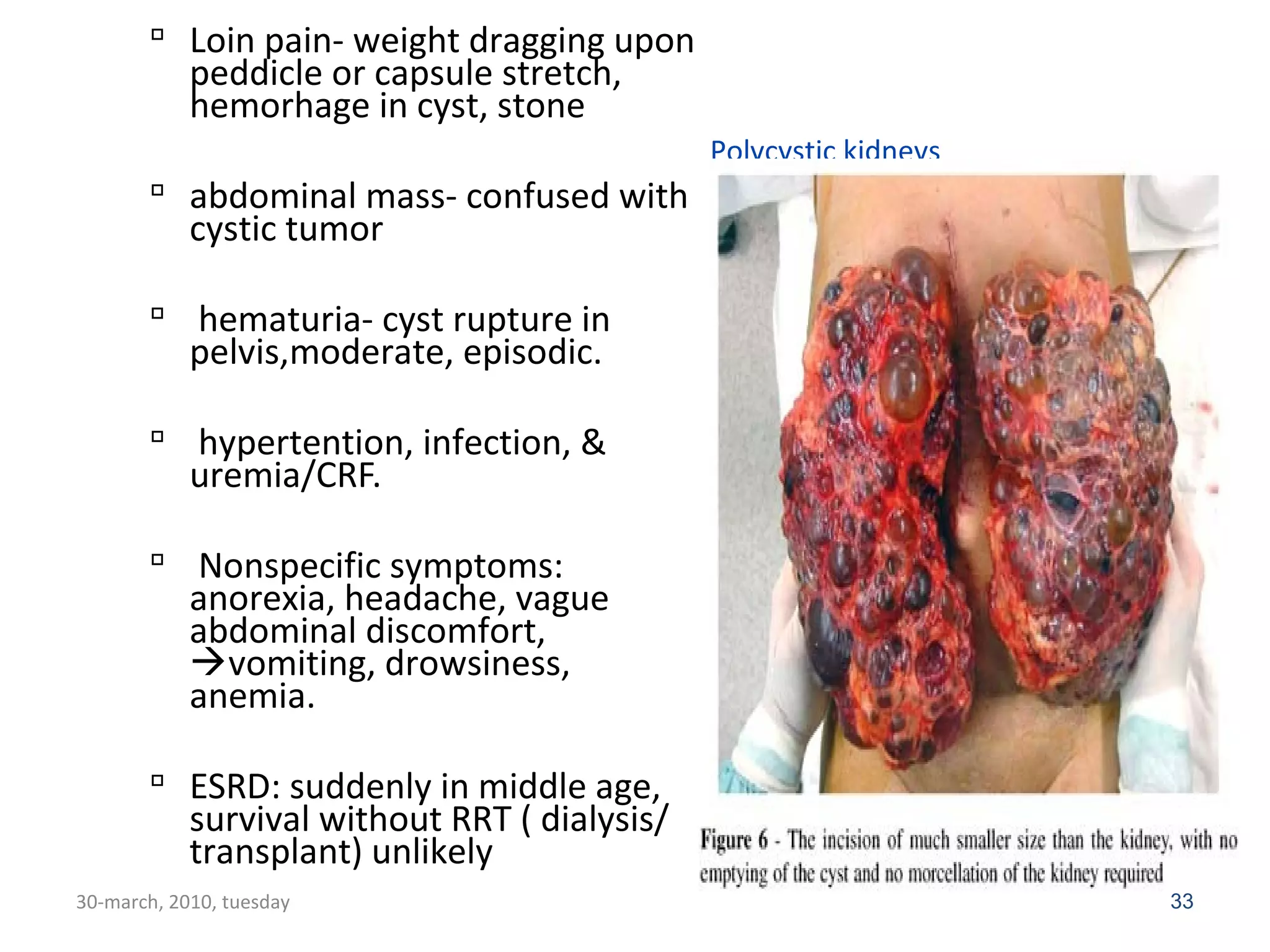
Polycystic kidneys
Loin pain- weight dragging upon
peddicle or capsule stretch,
hemorhage in cyst, stone
abdominal mass- confused with
cystic tumor
hematuria- cyst rupture in
pelvis,moderate, episodic.
hypertention, infection, &
uremia/CRF.
Nonspecific symptoms:
anorexia, headache, vague
abdominal discomfort,
vomiting, drowsiness,
anemia.
ESRD: suddenly in middle age,
survival without RRT ( dialysis/
transplant) unlikely
30-march, 2010, tuesday 33
Editor's Notes
#26 UBs sprout from the distal end of the mesonephric duct by week 5