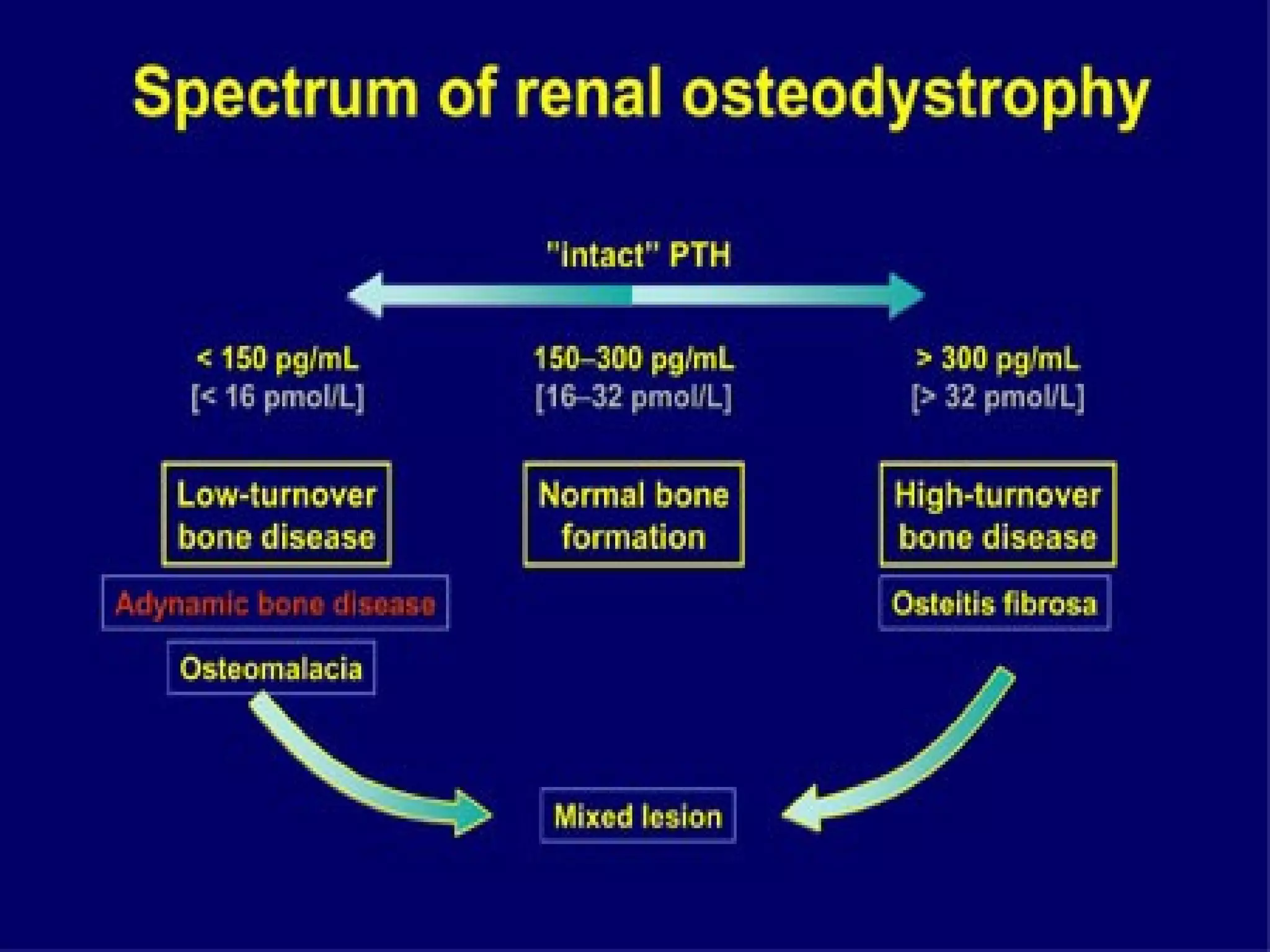
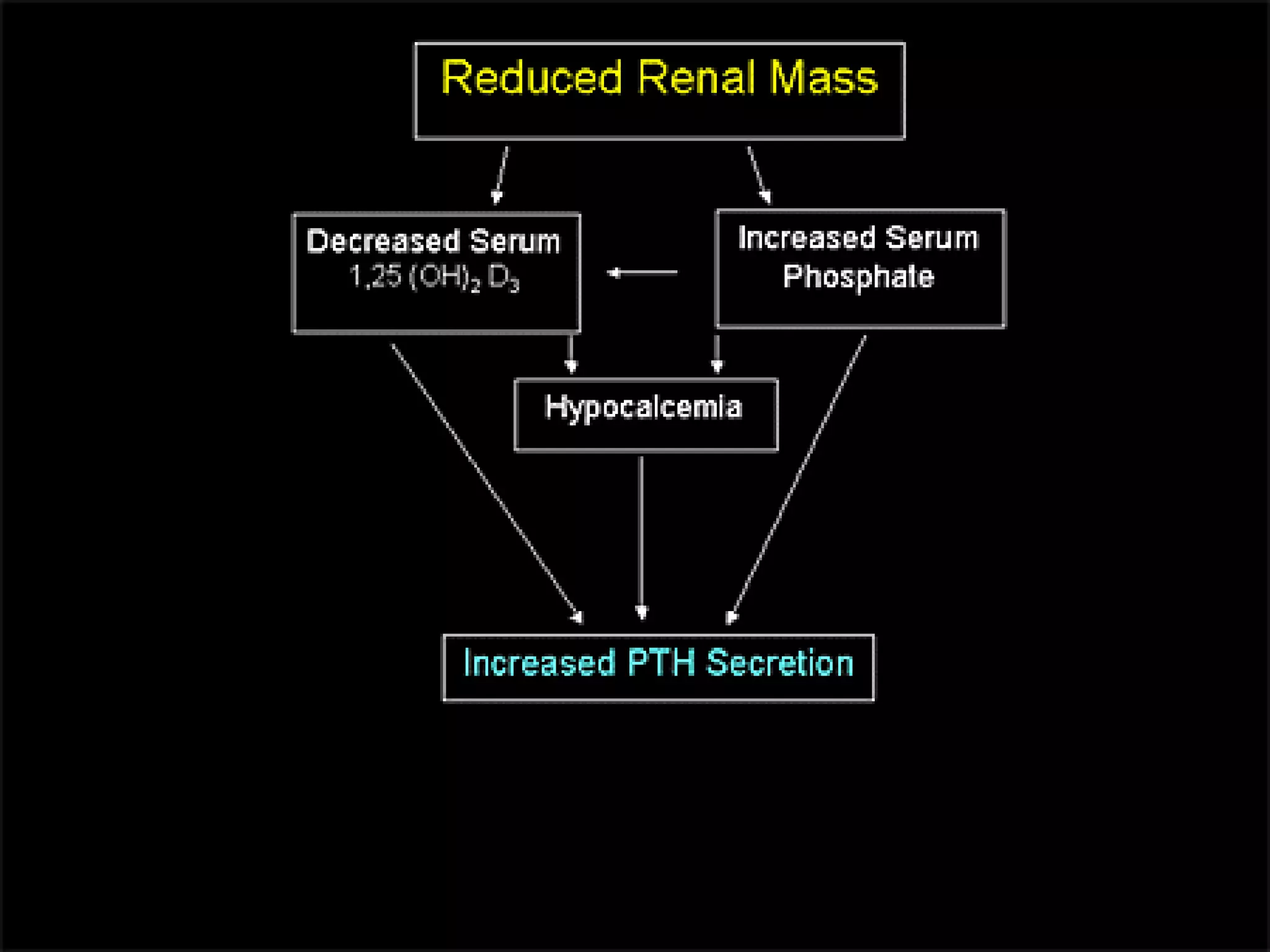
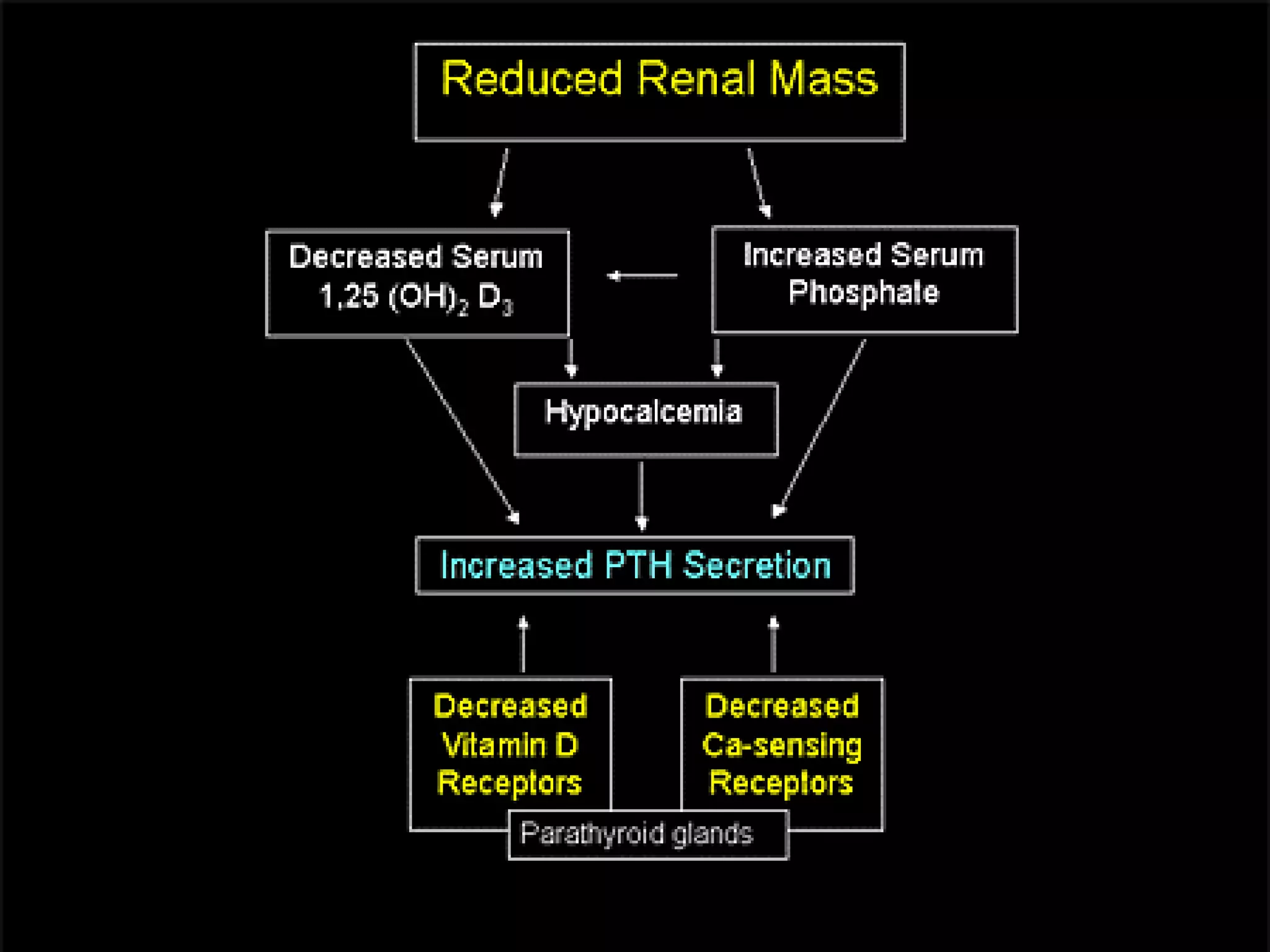


This document discusses bone and mineral disease in patients with chronic kidney disease. Key points: 1) Patients with chronic kidney disease often develop metabolic bone disease due to abnormalities in calcium, phosphorus, vitamin D, and parathyroid hormone levels. This can lead to bone abnormalities like osteitis fibrosa or adynamic bone. 2) Secondary hyperparathyroidism is common, driven by phosphorus retention, low vitamin D, and decreased calcium sensing by the parathyroid glands. High PTH then causes high bone turnover. 3) In addition to bone effects, extraskeletal calcification can occur in blood vessels, skin, and other tissues in patients with kidney disease. Care involves monitoring mineral
Introduction to metabolic bone diseases in CKD using a case of a 26-year-old male with ESRD.
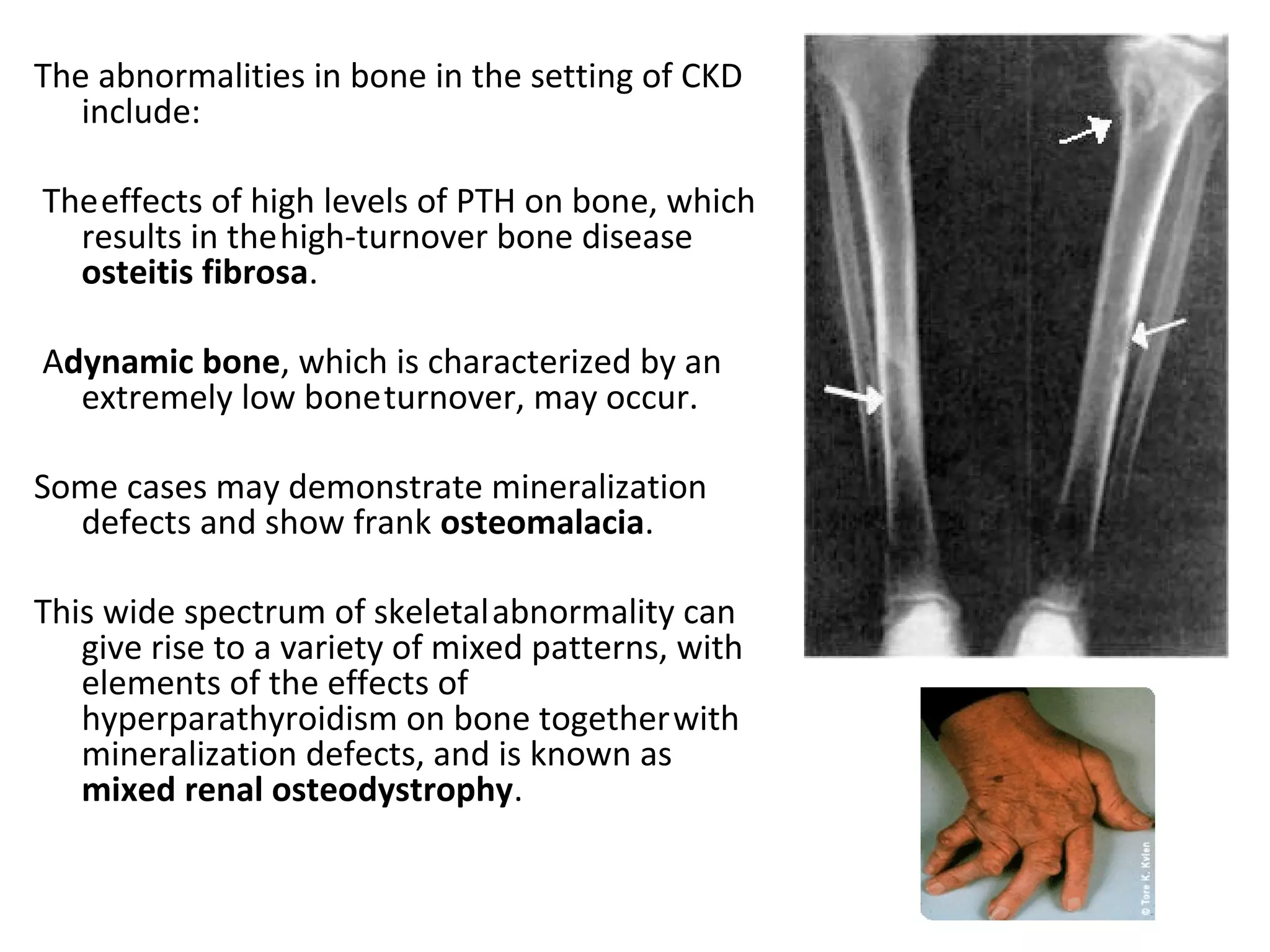
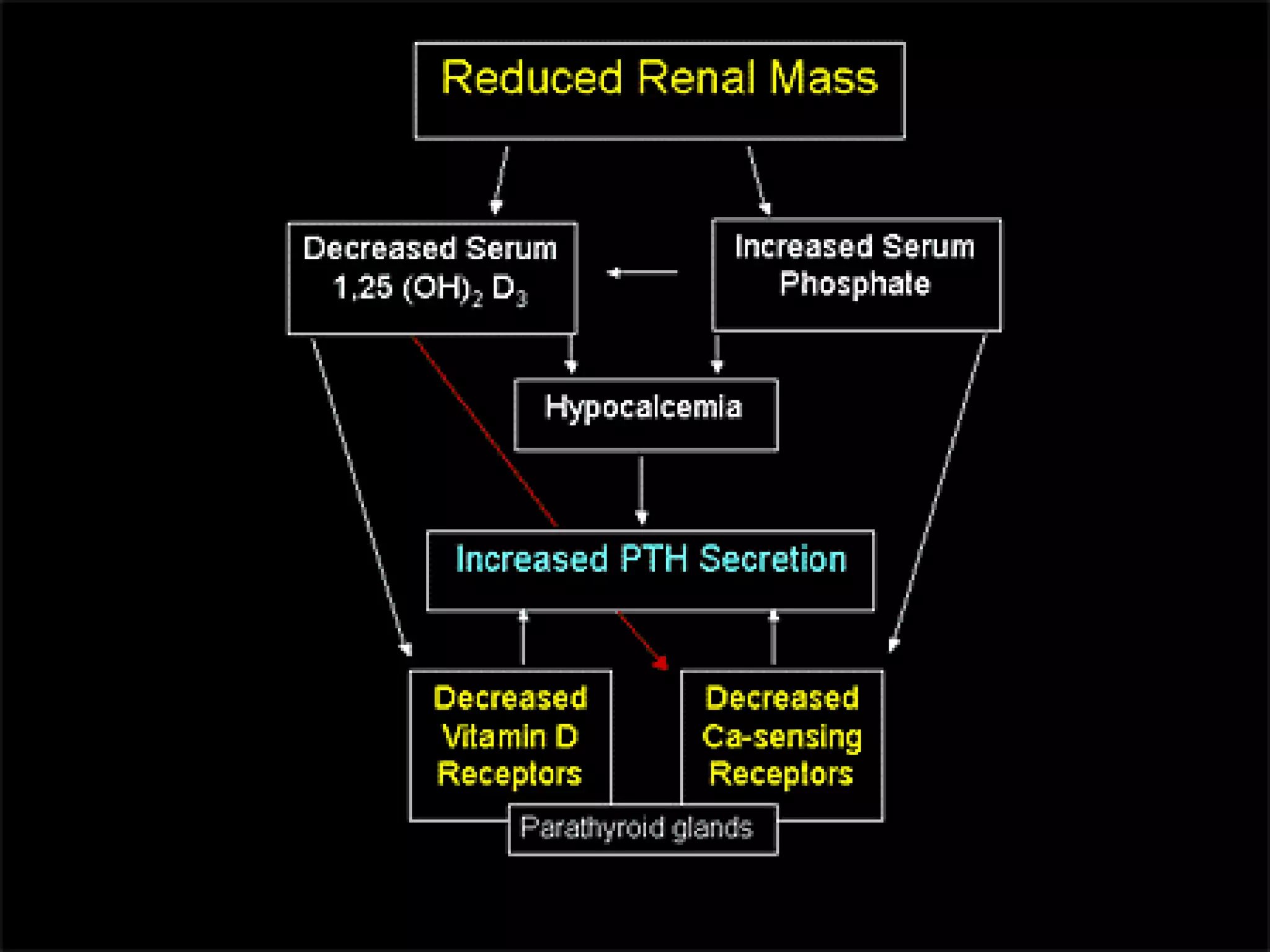
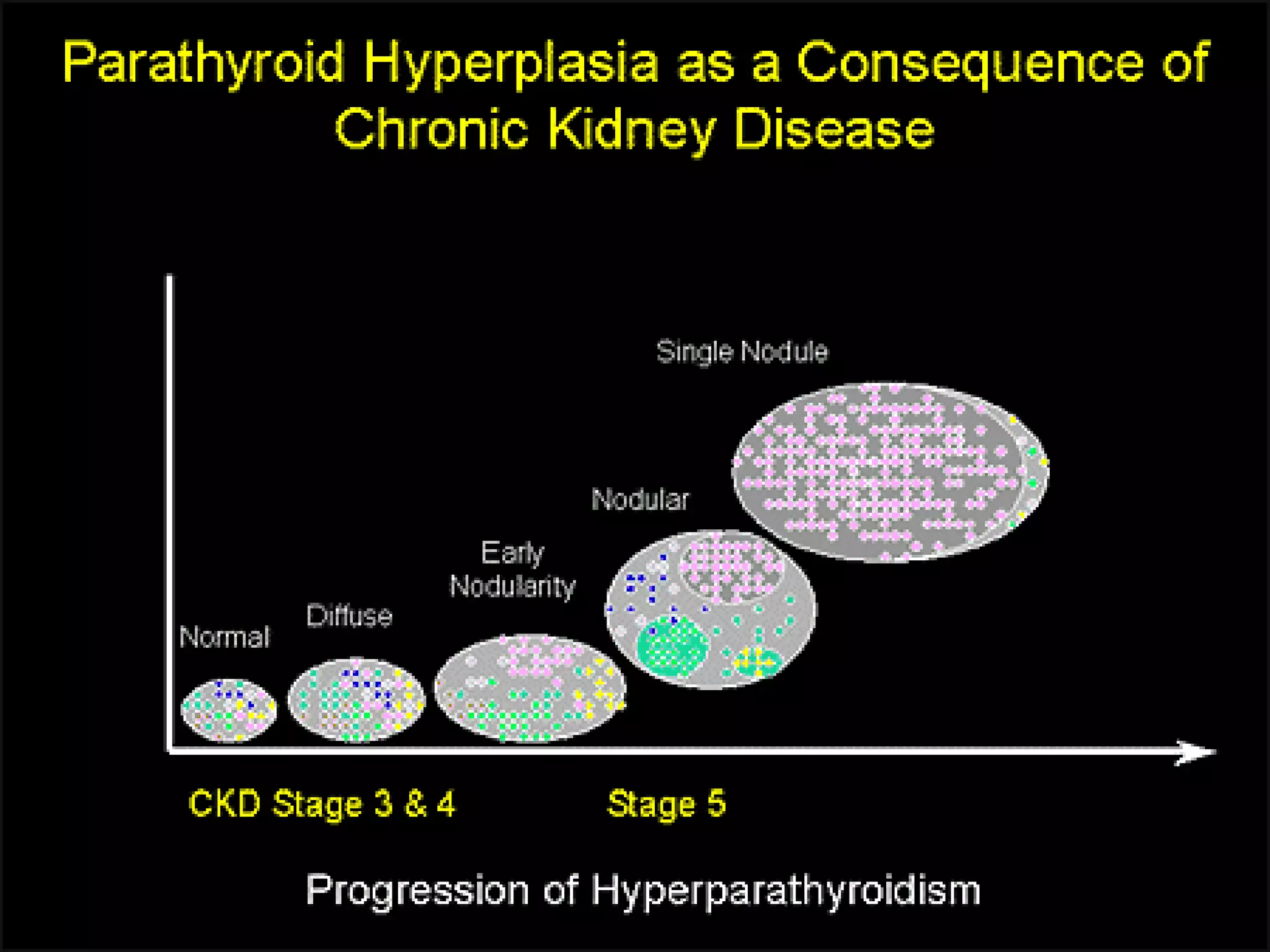
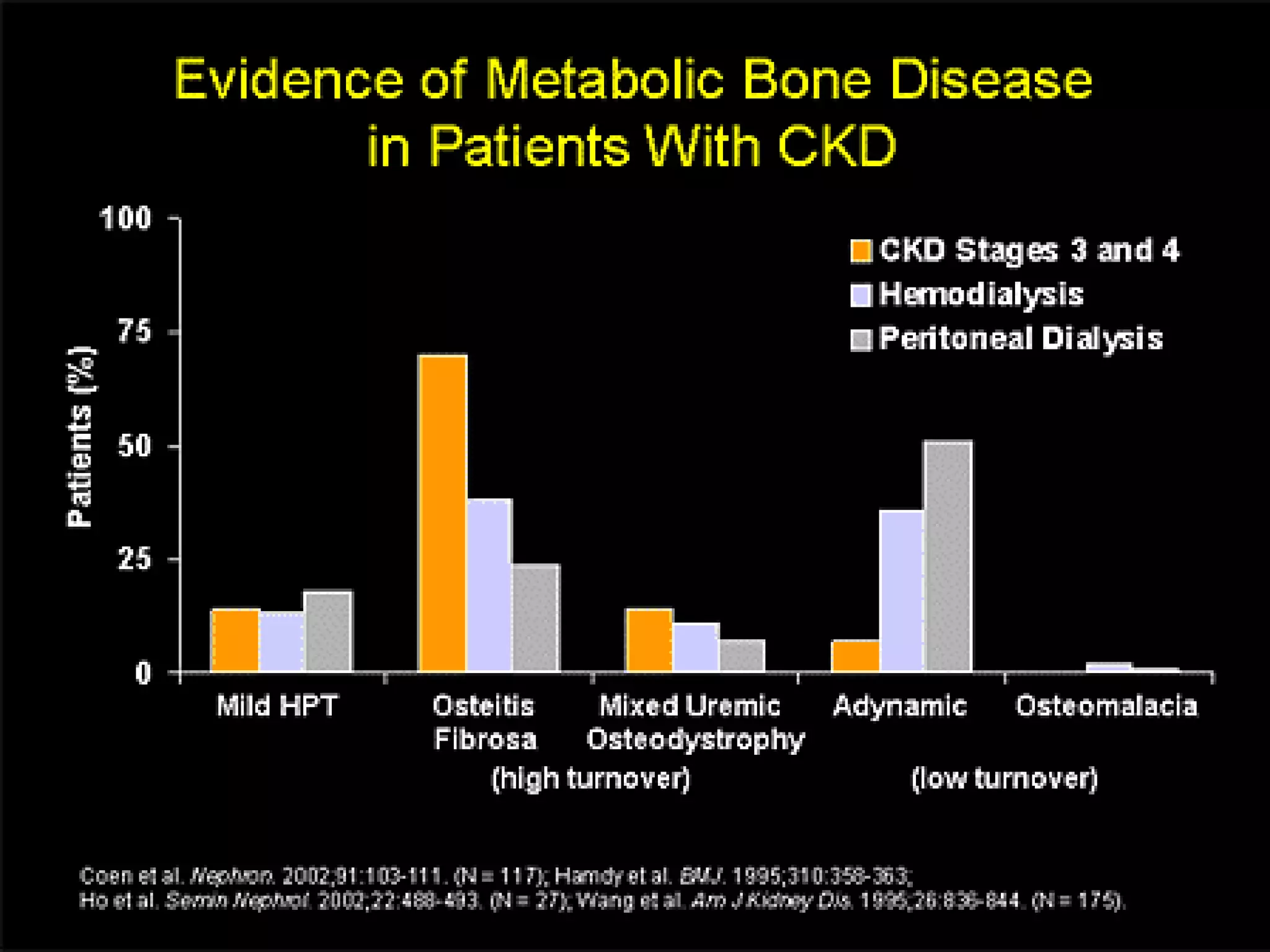
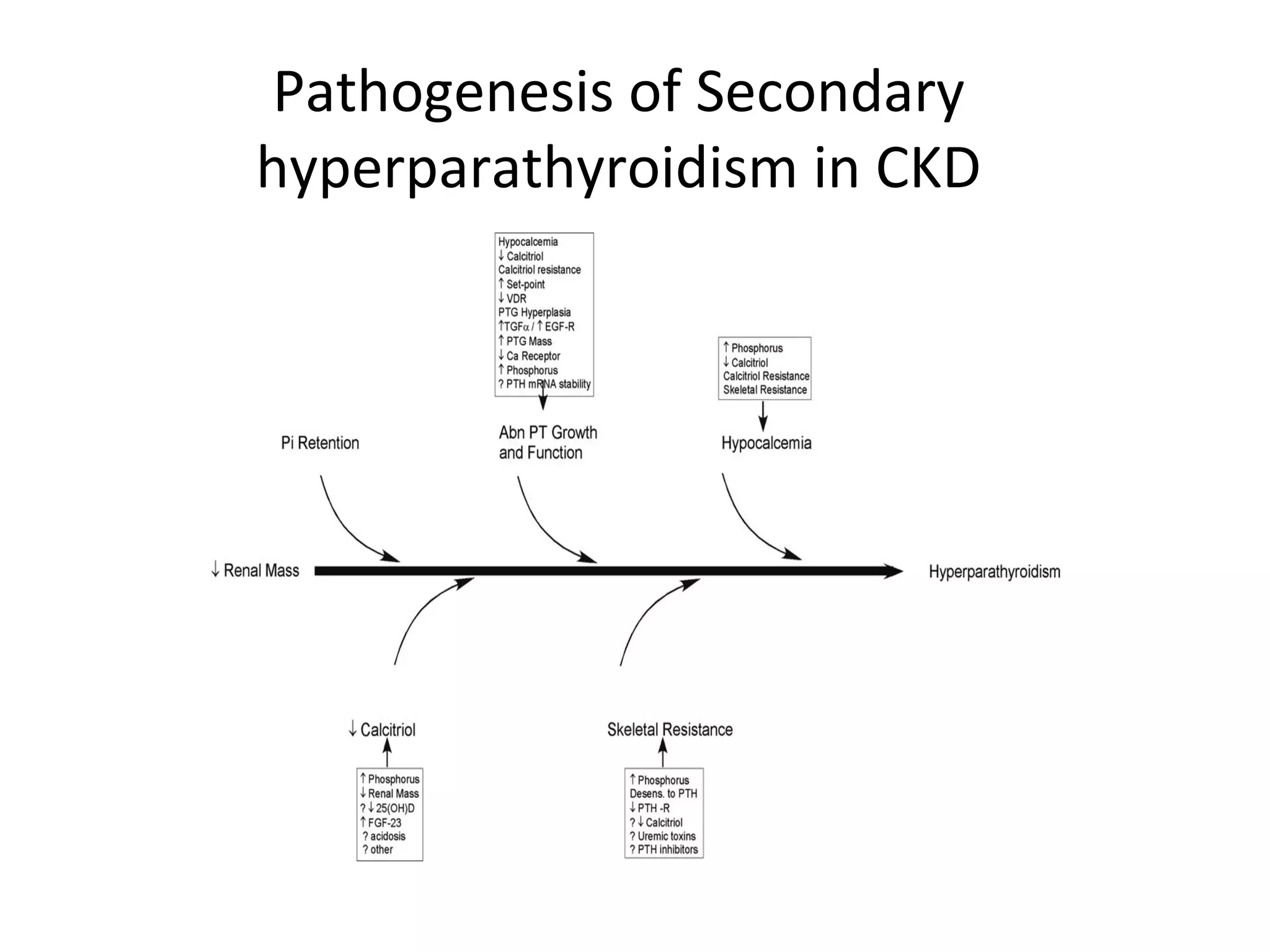
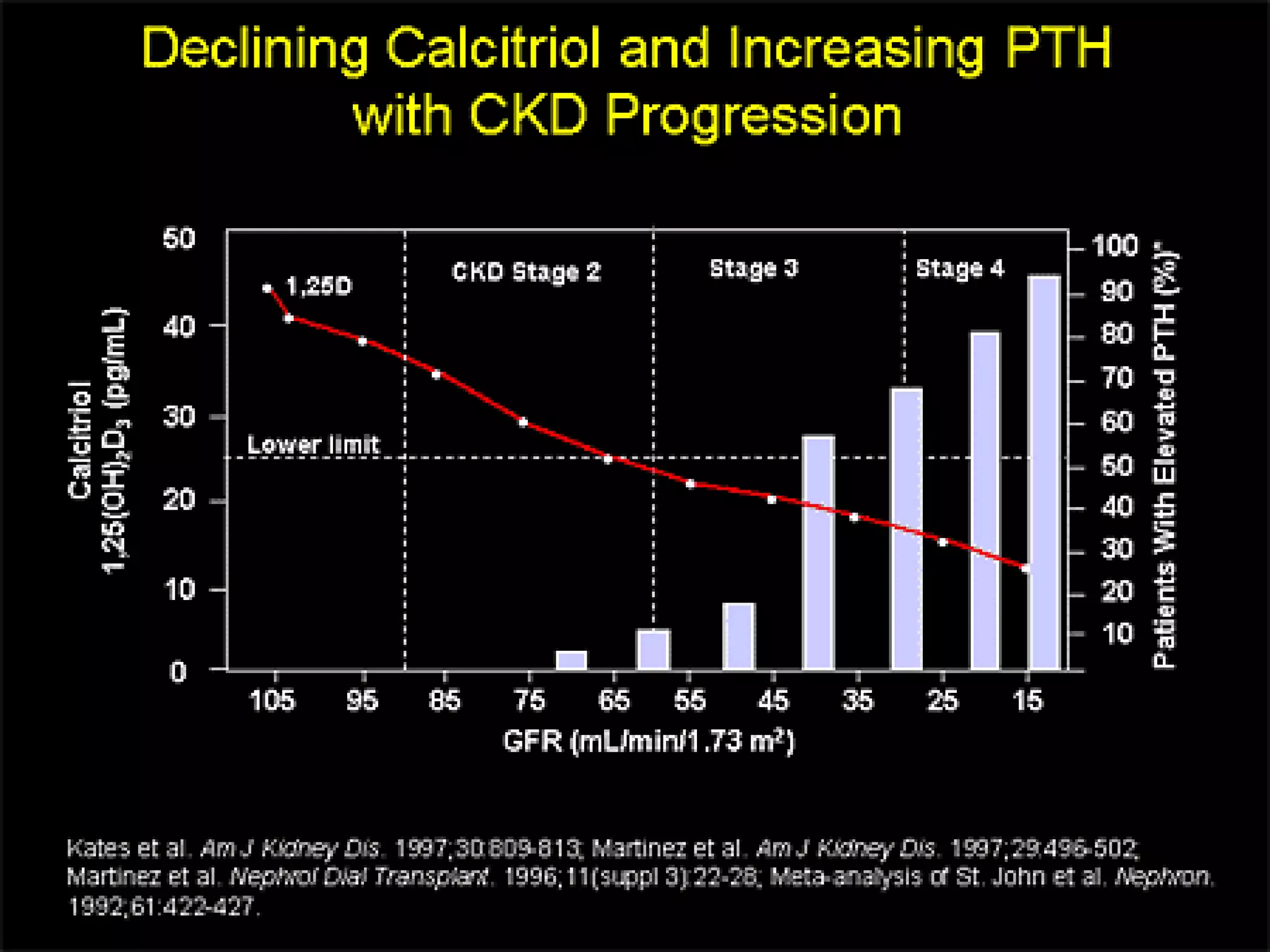
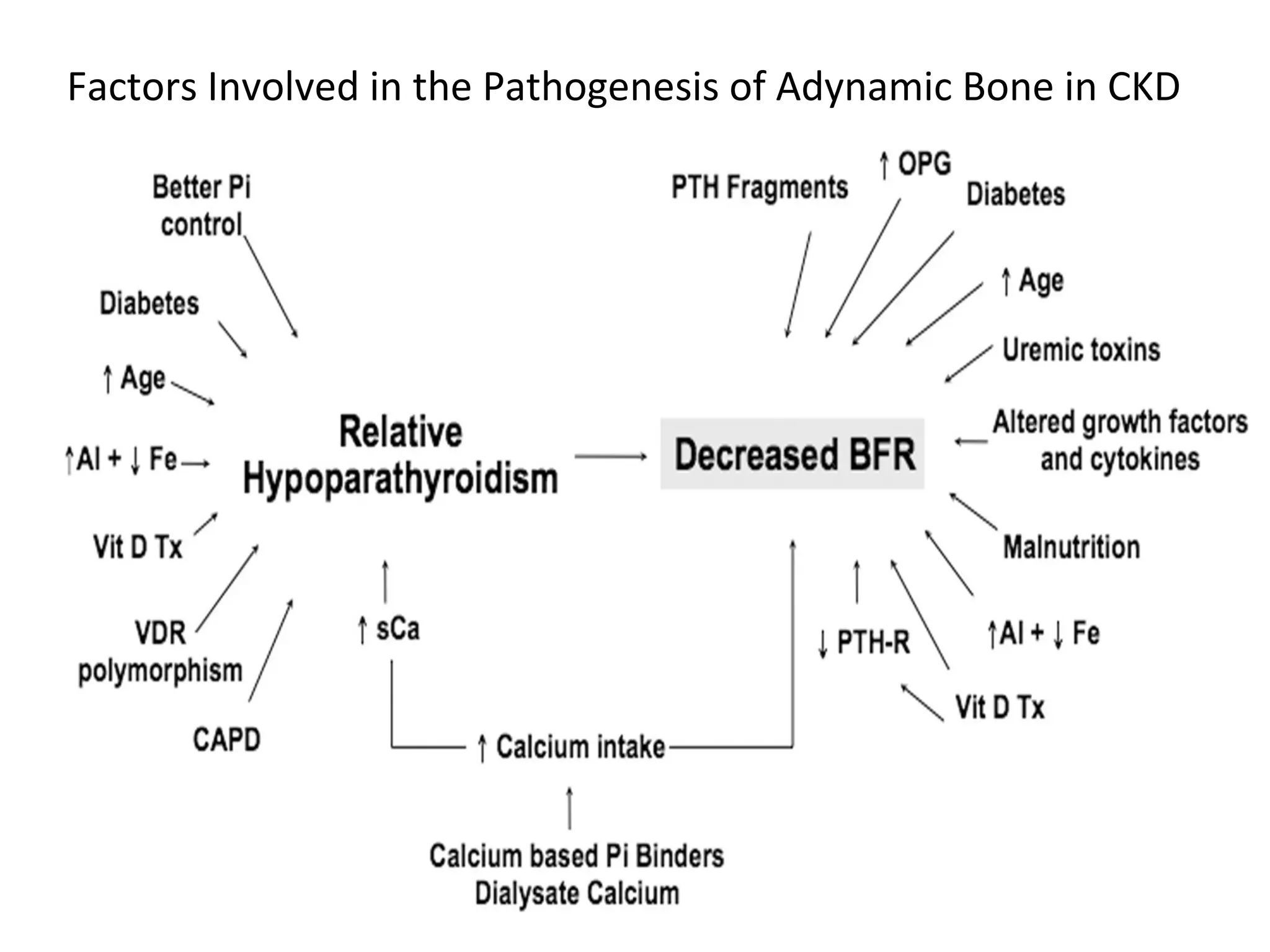
Focus on disease progression, emphasizing tertiary hyperparathyroidism and complications like fractures.Exploration of high-turnover conditions due to secondary hyperparathyroidism and calcium-phosphate dynamics.
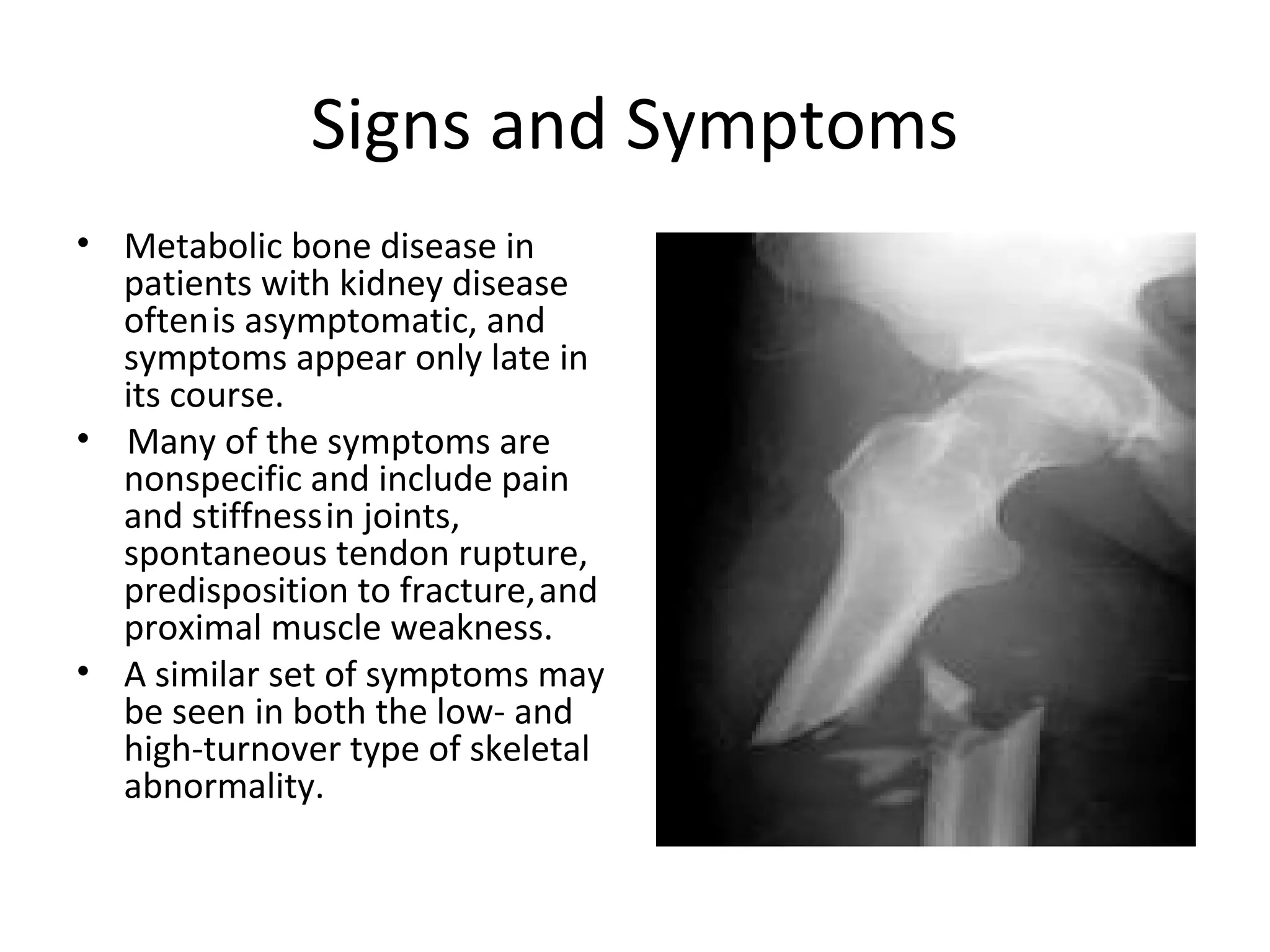
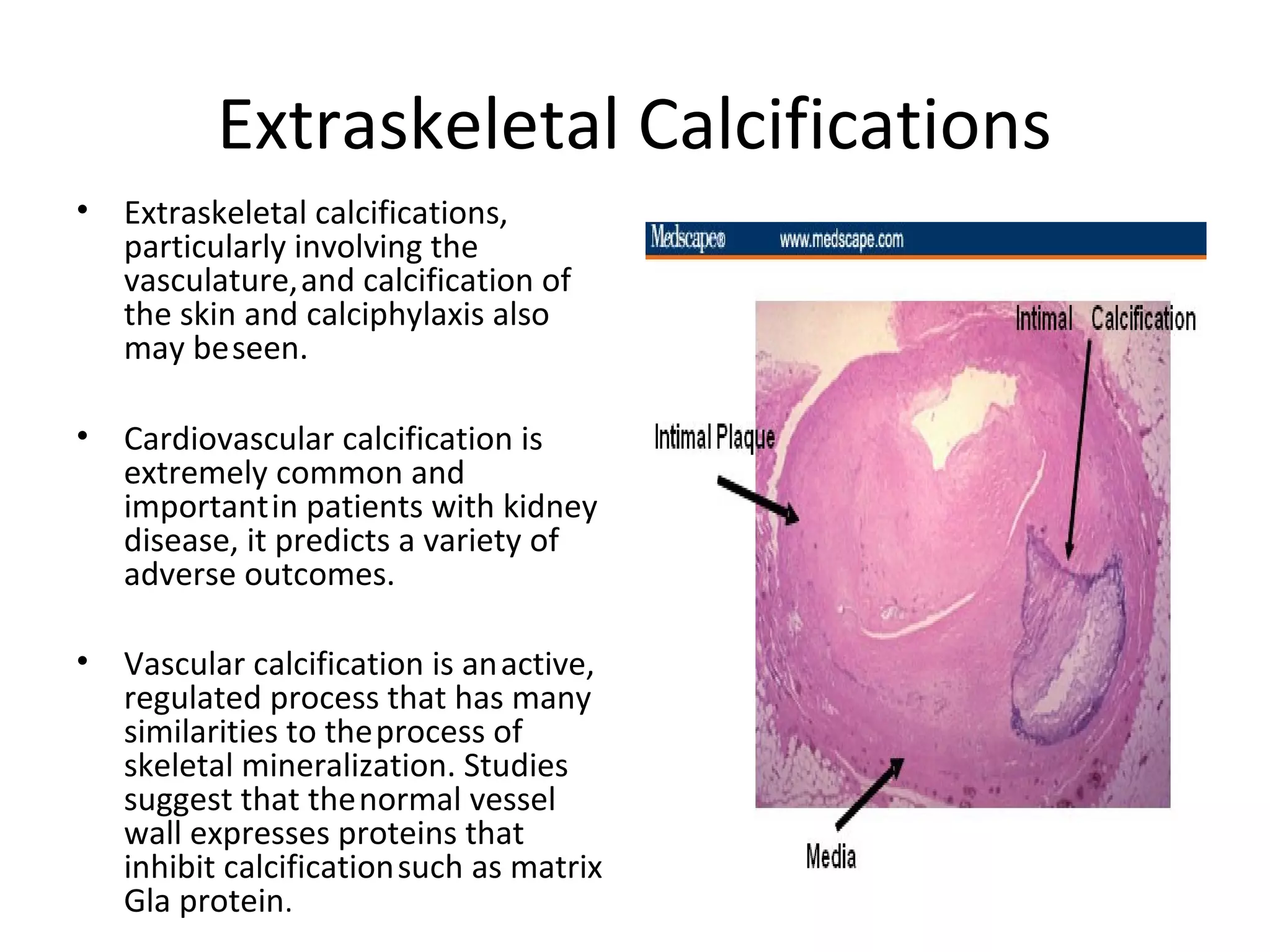
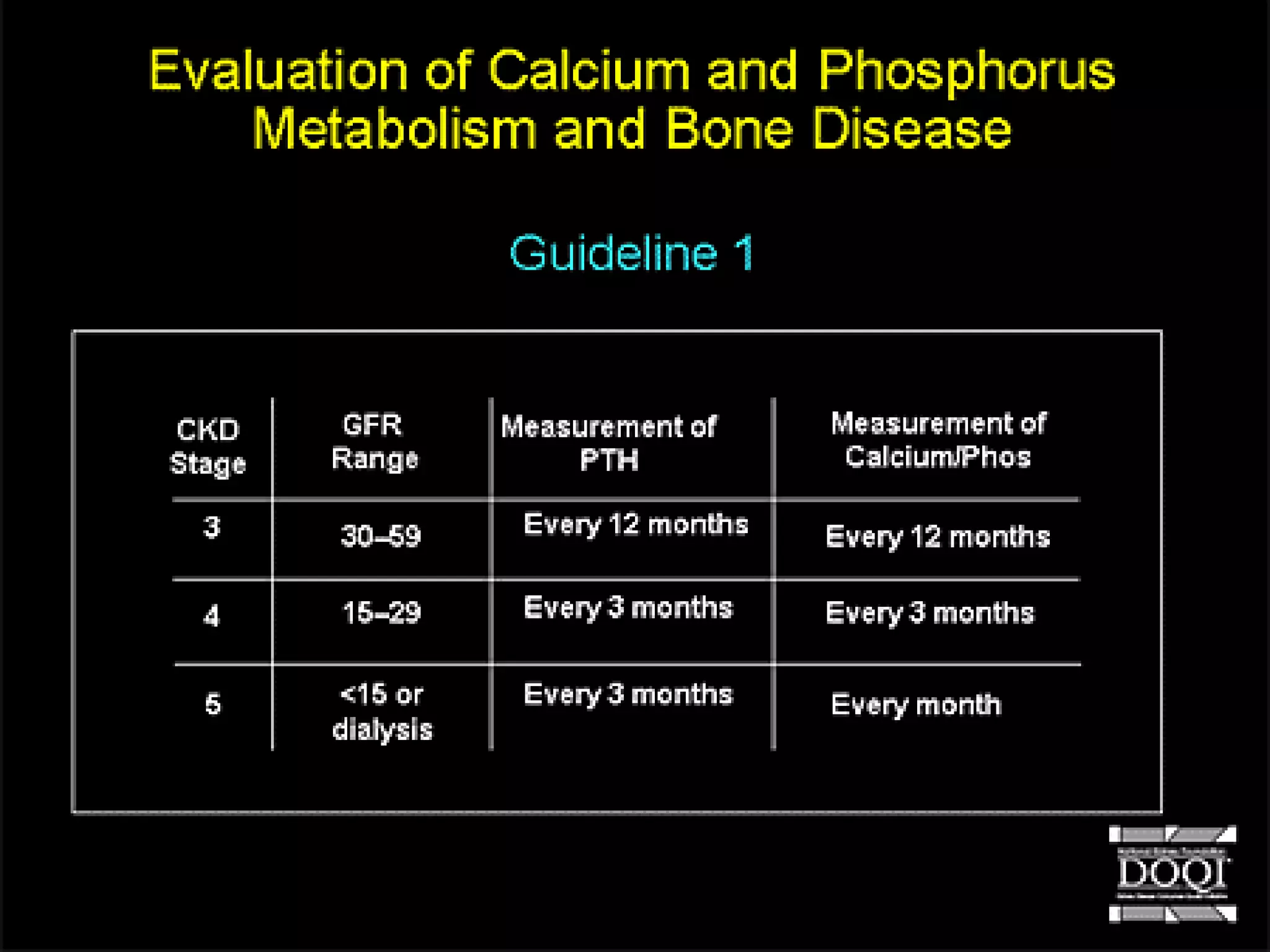
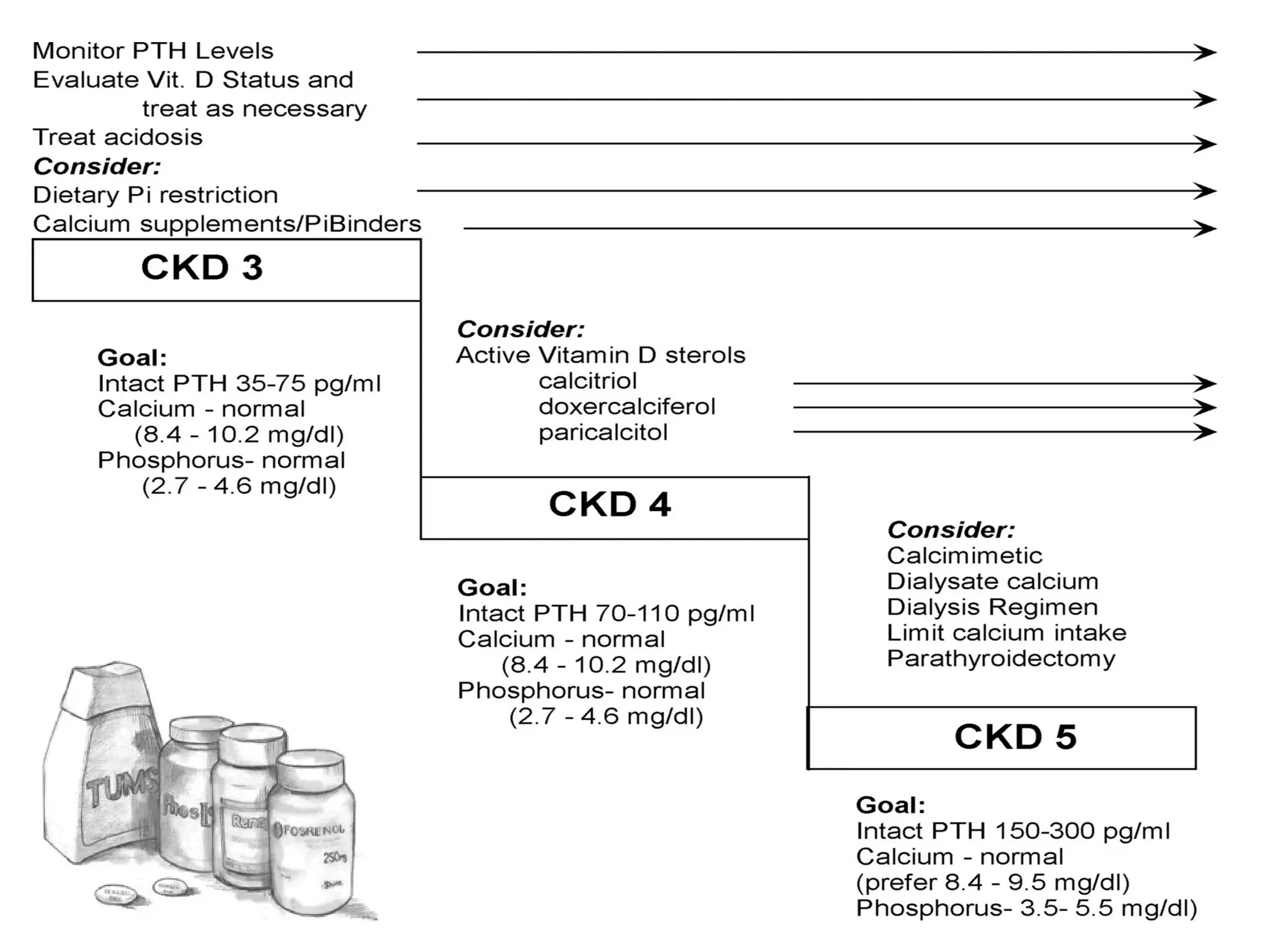
Discussion on signs and symptoms of metabolic bone disease in CKD patients along with management strategies.Outlines prevention methods for hyperparathyroidism and management of calcium and phosphorus levels.Citations of key studies and materials relevant to metabolic bone disease research and treatment.










































































































