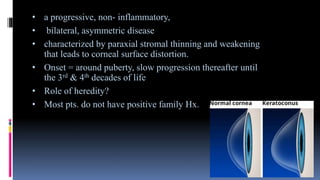
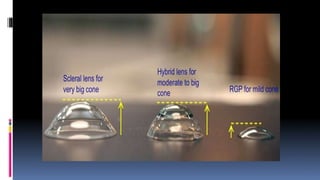
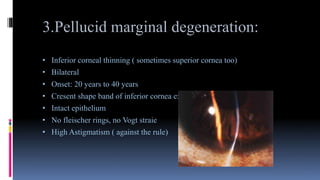
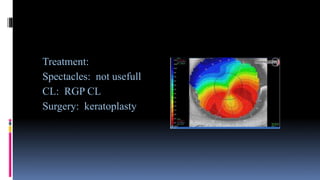
This document summarizes various congenital corneal abnormalities including microcornea, megalocornea, and cornea plana. It then discusses corneal ectasias like keratoconus, keratoglobus, and pellucid marginal degeneration. Keratoconus is characterized by thinning and distortion of the cornea and can be detected using tools like retinoscopy, slit lamp examination, and corneal topography. It progresses slowly from puberty to middle age. Treatments include spectacles, rigid gas permeable contact lenses, and keratoplasty. Keratoglobus involves generalized corneal thinning from birth. Pellucid marginal degeneration causes inferior corneal thinning in a crescent shape.












































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




