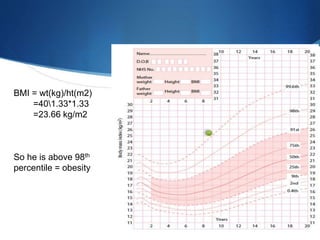
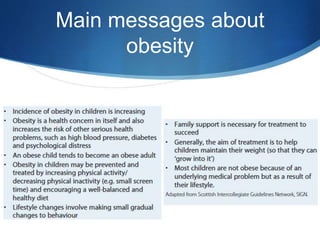
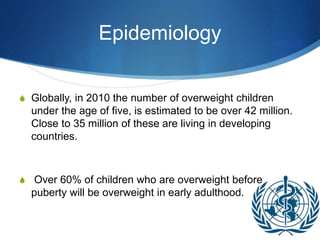
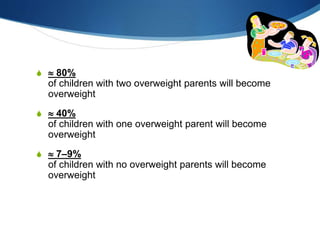
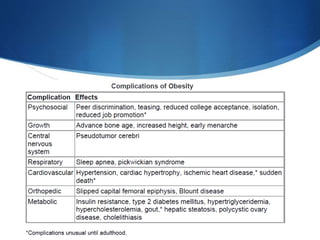
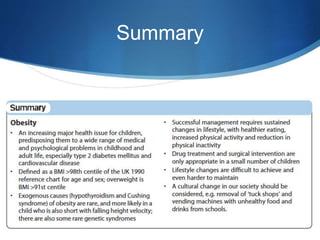
This document discusses pediatric obesity, including its definition using BMI, epidemiology, causes, complications, treatment, and prevention. Regarding definition and BMI, obesity in children is defined as excess body fat that negatively impacts health, and is diagnosed using BMI centiles where overweight is >91st centile and obese is >98th centile. The document then reviews the rising global rates of pediatric obesity and risk of obesity continuing into adulthood. Causes discussed include genetic predisposition and obesogenic environmental factors that promote overeating and sedentary behaviors. Complications can impact nearly every organ system, while treatment involves lifestyle changes and may include multidisciplinary programs depending on severity. Prevention strategies incorporate breastfeeding, appropriate portion sizes,