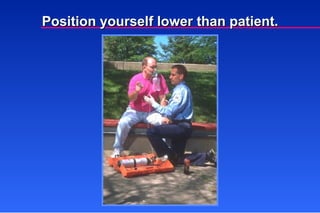
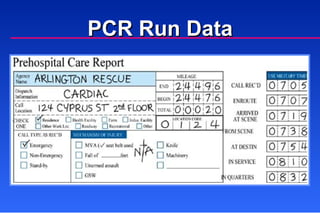
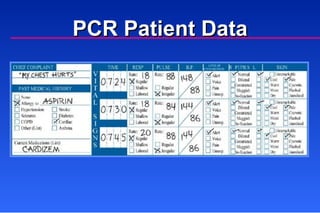
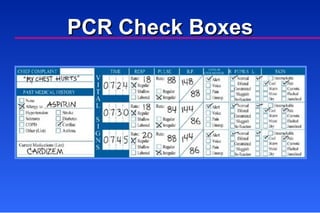
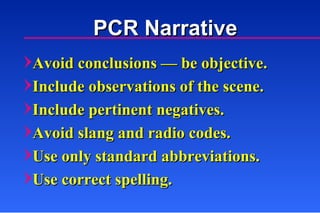
The document discusses principles of communication and documentation for patient care. It outlines the required elements of a radio report which include unit and provider level, estimated time of arrival, patient age and sex, chief complaint, history, vital signs, physical exam findings, treatment, and response to care. It also describes ways to improve interpersonal communication such as using clear language, maintaining eye contact, speaking slowly, and listening to the patient. Proper documentation is also covered, including the minimum data set required for a patient care report and correcting errors on documentation.

































![Chapter 016[1]](https://cdn.slidesharecdn.com/ss_thumbnails/chapter0161-120508224512-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)