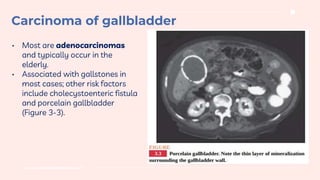
Cholangitis is an infection of the biliary tract typically caused by obstruction, with choledocholithiasis being a common culprit. The condition presents with symptoms like RUQ pain, jaundice, and fever, requiring immediate treatment, including IV antibiotics and potential biliary decompression. Gallbladder carcinoma is often associated with gallstones, presents with nonspecific symptoms, and has a poor prognosis, with over 90% mortality within a year due to late detection.





































![Surgery cholangitis[1]](https://cdn.slidesharecdn.com/ss_thumbnails/surgery-cholangitis1-120601032247-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)





















































