INTRODUCTION
Cholecystitis is theacute or chronic inflammation
of the gallbladder. It normally happens because a
gallstone gets stuck at the opening of the
gallbladder. It can lead to fever, pain, nausea, and
severe complications.
1.Calculous cholecystitis: Incalculous cholecystitis, a gallbladder stone
obstructs bile outflow.
2.Acalculous cholecystitis: Acute inflammation in the absence of
obstruction by gallstones.
3.Acute cholecystitis: This inflammation often causes severe pain in the mid
or right upper abdomen. Pain can also spread between the shoulder blades. In
severe cases, the gallbladder may tear or burst and release bile into the
abdomen, causing severe pain. This can be a life-threatening situation that
requires immediate attention.
4.Chronic cholecystitis: Recurrent bouts of mild swelling and
irritation/inflammation will often damage the wall of the gallbladder causing it
to thicken, shrink and lose proper function.
5.
Pathophysiology
Obstruction. Calculouscholecystitis occurs when a gallbladder stone
obstructs the bile outflow.
Chemical reaction. Bile remaining in the gallbladder initiates a
chemical reaction; autolysis and oedema occur.
Compression. Blood vessels in the gallbladder compressed,
compromising its vascular supply.
6.
Causes
Gallbladder stone.Most often, cholecystitis is the result of hard particles
that develop in your gallbladder (gallstones). Gallstones can block the
tube (cystic duct) through which bile flows when it leaves the gallbladder.
Bile builds up, causing inflammation.
Bacteria. Bacteria plays a minor role in cholecystitis; E. coli, Klebsiella,
Streptococcus, and Clostridium species.
Alterations in fluids and electrolytes. Acalculous cholecystitis is
speculated to be caused by alterations in fluids and electrolytes.
Bile stasis. Bile stasis or the lack of gallbladder contraction also play a
role in the development of cholecystitis.
7.
CONTD…
•Tumor. A tumormay prevent bile from draining out of gallbladder properly,
causing bile buildup that can lead to cholecystitis.
•Infection. AIDS and certain viral infections can trigger gallbladder inflammation.
•Blood vessel problems. A very severe illness can damage blood vessels and
decrease blood flow to the gallbladder, leading to cholecystitis.
CONTD…
Murphy sign:A Murphy sign is a “catch” in the breath elicited by gently pressing on the right upper quadrant and
asking the patient to take a deep breath. Patient will have pain during inhalation.
Boas sign: Boas' or Boas sign is hyperesthesia (increased or altered sensitivity) below the right scapula can be a
symptom in acute cholecystitis (inflammation of the gallbladder). Originally this sign referred to point tenderness
in the region to the right of the 9th to 11th thoracic vertebrae.
Mirrizi syndrome: defined as common hepatic duct obstruction caused by extrinsic compression from an impacted stone in
the cystic duct or infundibulum of the gallbladder . Patients with Mirizzi syndrome can present with jaundice, fever, and right
upper quadrant pain.
Charcot's cholangitis triad: is the combination of jaundice; fever, usually with rigors; and right upper
quadrant abdominal pain. It occurs as a result of ascending cholangitis (an infection of the bile duct in the liver).
Courvoisier's law (or courvoisier syndrome, or courvoisier's sign or courvoisier-terrier's sign): states that in
the presence of a palpable enlarged gallbladder which is non-tender and accompanied with mild painless jaundice, the cause is
unlikely to be gallstones.
Reynolds pentad: collection of signs and symptoms suggesting the diagnosis obstructive ascending cholangitis, a
serious infection of the biliary system. It is a combination of Charcot's triad (right upper quadrant pain,
jaundice, and fever) with shock (low blood pressure, tachycardia) and an altered mental status.
11.
Complications
Cholecystitis can progressto gallbladder complications, such as:
Empyema. An empyema of the bladder develops if the gallbladder becomes filled with
purulent fluid.
Gangrene. Gangrene develops because the tissues do not receive enough oxygen and
nourishment at all.
Cholangitis. The infection progresses as it reaches the bile duct.
• Infection within the gallbladder. If bile builds up within gallbladder, causing
cholecystitis, the bile may become infected.
• Torn gallbladder. A tear (perforation) in gallbladder may result from gallbladder swelling,
infection or death of tissue.
12.
Assessment and DiagnosticFindings
Biliary ultrasound: Reveals calculi, with gallbladder and/or bile duct distension (frequently the initial diagnostic procedure).
Oral cholecystography (OCG): Preferred method of visualizing general appearance and function of gallbladder, including
presence of filling defects, structural defects, and/or stone in ducts/biliary tree. Can be done IV (IVC) when nausea/vomiting
prevent oral intake, when the gallbladder cannot be visualized during OCG, or when symptoms persist following
cholecystectomy. IVC may also be done perioperatively to assess structure and function of ducts, detect remaining stones after
lithotripsy or cholecystectomy, and/or to detect surgical complications. Dye can also be injected via T-tube drain
postoperatively.
Endoscopic retrograde cholangiopancreatography (ERCP): Visualizes biliary tree by cannulation of the common bile duct
through the duodenum. Assess the retroperitoneal organs gallbladder, bile duct and pancreas.
Percutaneous transhepatic cholangiography (PTC): Fluoroscopic imaging distinguishes between gallbladder disease
and cancer of the pancreas (when jaundice is present); supports the diagnosis of obstructive jaundice and reveals calculi in
ducts.
Cholecystograms (for chronic cholecystitis): Reveals stones in the biliary system. Note: Contraindicated in acute
cholecystitis because patient is too ill to take the dye by mouth.
13.
CONTD…
Nonnuclear CTscan: May reveal gallbladder cysts, dilation of bile ducts, and distinguish between
obstructive/nonobstructive jaundice.
Hepatobiliary (HIDA, PIPIDA) scan: May be done to confirm diagnosis of cholecystitis, especially when
barium studies are contraindicated. Scan may be combined with cholecystokinin injection to demonstrate
abnormal gallbladder ejection. Done to evaluate the health and function of gall bladder.
Abdominal x-ray films (multilocational): Radiopaque (calcified) gallstones present in 10%–15% of cases;
calcification of the wall or enlargement of the gallbladder.
CBC: leucocytosis.
Serum bilirubin and amylase: Elevated.
14.
CONTD…
Serum liverenzymes—AST; ALT; ALP; LDH: Slight elevation; alkaline phosphatase
and 5-nucleotidase are markedly elevated in biliary obstruction.
Prothrombin levels: Reduced when obstruction to the flow of bile into the intestine
decrease’s absorption of vitamin K.
Ultrasonography. Ultrasound is the preferred initial imaging test for the diagnosis of
acute cholecystitis; scintigraphy is the preferred alternative.
CT scan. CT scan is a secondary imaging test that can identify extra-biliary disorders
and acute complications of cholecystitis.
15.
Contd…
MRI. Magneticresonance imaging is also a possible secondary choice for confirming a
diagnosis of acute cholecystitis.
Oral cholecystography. Preferred method of visualizing general appearance and function
of the gallbladder.
Cholecystogram. Cholecystography reveals stones in the biliary system.
Abdominal x-ray. Radiopaque or calcified gallstones present in 10% to 15% of cases.
16.
Management:
Management may involvecontrolling the signs and symptoms and the inflammation of
the gallbladder.
Fasting. The patient may not be allowed to drink or eat at first in order to take the
stress off the inflamed gallbladder; IV fluids are prescribed to provide temporary food
for the cells.
Supportive medical care. This may include restoration pf hemodynamic
stability and antibiotic coverage for gram-negative enteric flora.
Gallbladder stimulation. Daily stimulation of gallbladder contraction with IV
cholecystokinin may help prevent the formation of gallbladder sludge in patients
receiving TPN.
17.
Pharmacologic Therapy:
The followingmedications may be useful in patients with cholecystitis:
Antibiotic therapy. Levofloxacin and Metronidazole for prophylactic
antibiotic coverage against the most common organisms.
Promethazine or Prochlorperazine may control nausea and prevent fluid
and electrolyte disorders.
Oxycodone or Acetaminophen may control inflammatory signs and
symptoms and reduce pain.
18.
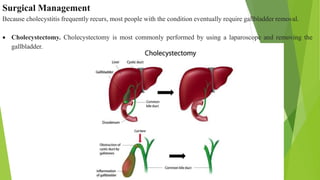
Surgical Management
Because cholecystitisfrequently recurs, most people with the condition eventually require gallbladder removal.
Cholecystectomy. Cholecystectomy is most commonly performed by using a laparoscope and removing the
gallbladder.
19.
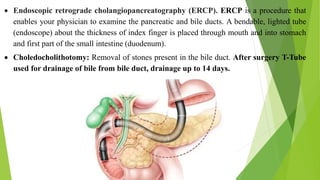
Endoscopic retrogradecholangiopancreatography (ERCP). ERCP is a procedure that
enables your physician to examine the pancreatic and bile ducts. A bendable, lighted tube
(endoscope) about the thickness of index finger is placed through mouth and into stomach
and first part of the small intestine (duodenum).
Choledocholithotomy: Removal of stones present in the bile duct. After surgery T-Tube
used for drainage of bile from bile duct, drainage up to 14 days.