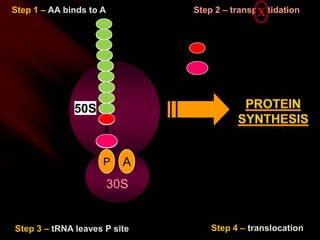
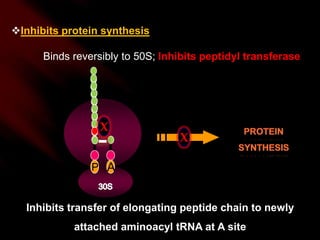
Chloramphenicol is a broad-spectrum bacteriostatic and bactericidal antibiotic. It inhibits bacterial protein synthesis by binding reversibly to the 50S subunit of the bacterial ribosome, inhibiting peptidyl transferase and preventing the transfer of elongating peptide chains. While effective against a variety of bacteria, it can cause serious and sometimes fatal side effects like bone marrow suppression and gray baby syndrome in neonates due to immature drug metabolism pathways. As a result, it is now rarely used due to toxicity concerns and the availability of alternative antibiotics.







































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
