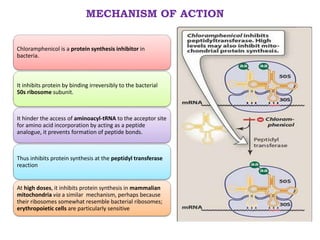
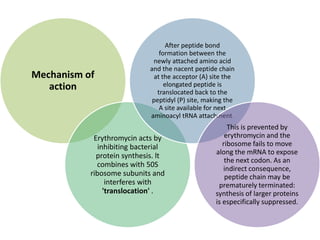
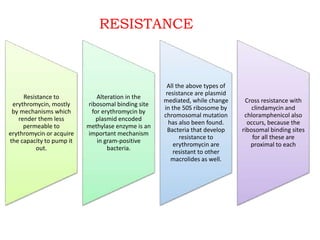
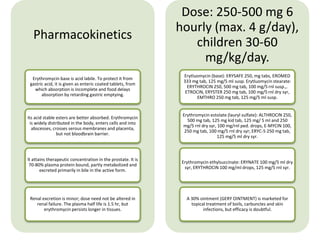
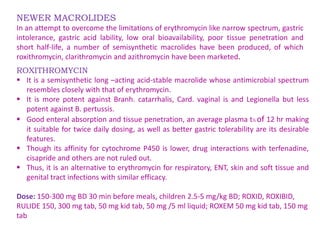
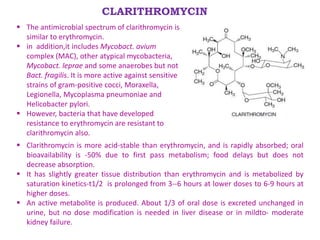
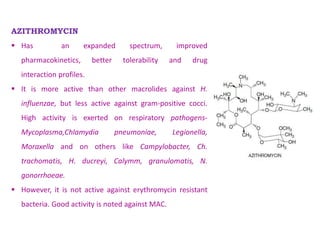
The document discusses antimicrobials, particularly antibiotics like chloramphenicol and macrolides, which are designed to inhibit or kill infecting organisms while minimizing effects on the host. Antibiotics work by targeting specific components of microbes or their metabolic processes, with chloramphenicol being a broad-spectrum protein synthesis inhibitor derived from Streptomyces venezuelae. Macrolides, including erythromycin, are characterized by a macrocyclic lactone structure and primarily serve as bacteriostatic agents through the inhibition of protein synthesis.


























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



