Downloaded 679 times

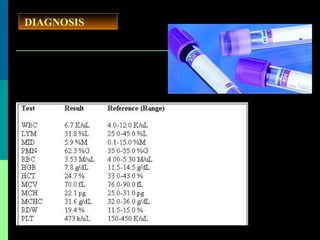



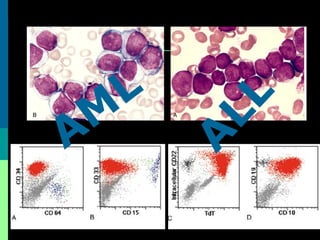
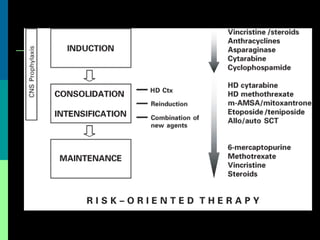

The document discusses acute lymphoblastic leukemia (ALL), which is the most common childhood leukemia. It makes up around 80% of childhood leukemia cases. The document covers the introduction, classification, etiology, diagnosis, clinical presentation, and treatment of ALL. It notes that the cure rate for ALL is around 85% with current treatments involving remission induction, intensification, and maintenance therapy. Prognosis depends on factors like age, white blood cell count at diagnosis, and the ALL subtype.




















































































