Download to read offline

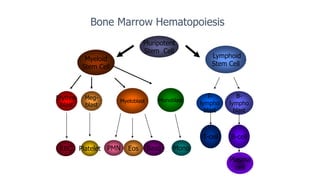



Leukemia is a group of cancers that affect the blood and bone marrow. This document discusses the main types of leukemia: 1. Acute myelogenous leukemia (AML) is characterized by increased proliferation of immature myeloid cells in the bone marrow. It accounts for about one-third of adult leukemias. 2. Acute lymphoblastic leukemia (ALL) is most common in children and is characterized by increased lymphoblasts in the bone marrow. About 85% of ALL cases are B-cell ALL. 3. Chronic myelogenous leukemia (CML) is a myeloproliferative neoplasm characterized by increased and unregulated growth of predominantly granulocytic























































































