Downloaded 57 times


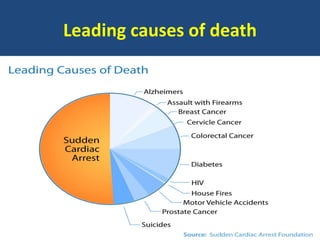


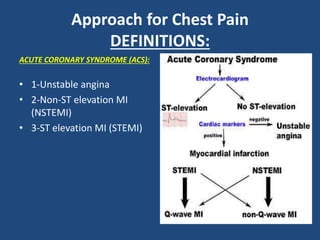
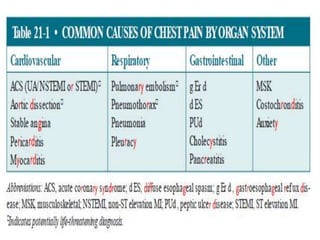


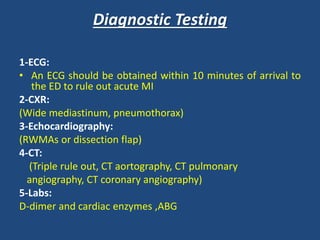
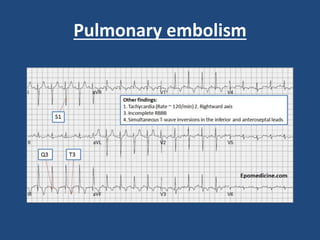
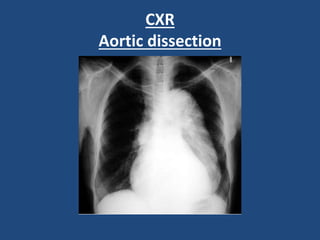
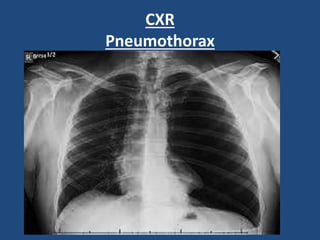
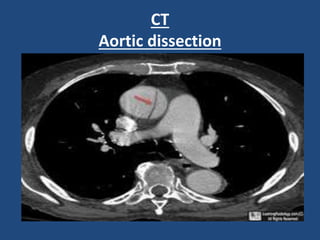
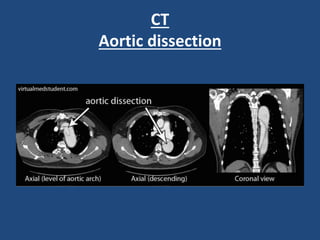
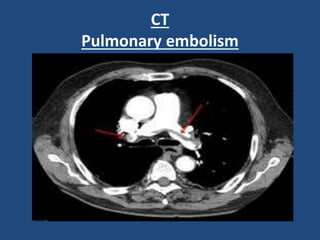
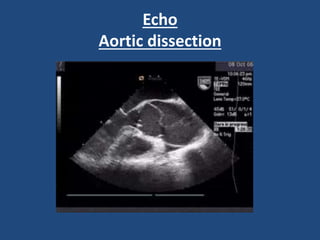


This document provides guidance on evaluating and managing common cardiovascular emergencies. It outlines the leading causes of cardiovascular emergencies, including acute chest pain, dyspnea, syncope, and hemodynamic instability. For patients presenting with chest pain, the priority is to differentiate life-threatening etiologies like pulmonary embolism, acute coronary syndrome, and aortic dissection from less serious conditions. The initial evaluation involves obtaining vital signs, performing a physical exam, 12-lead ECG, chest x-ray, and cardiac biomarker tests. Emergent conditions require urgent diagnostic testing and treatment to reduce mortality. Timely diagnosis and management is critical for improving outcomes in cardiovascular emergencies.



































































