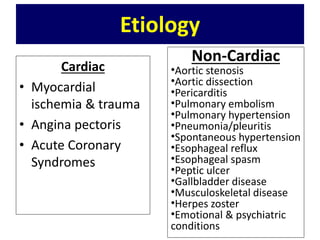
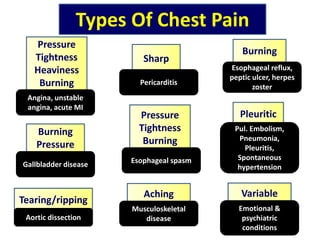
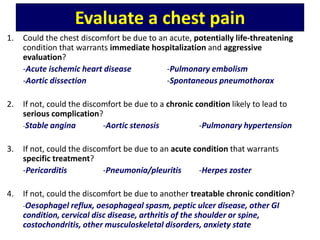
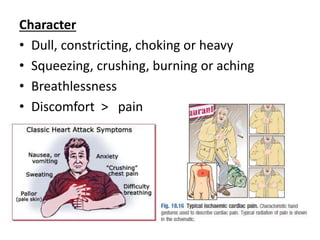
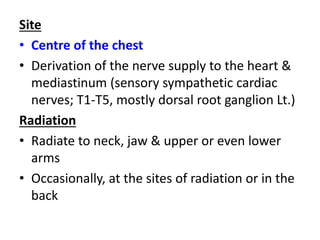
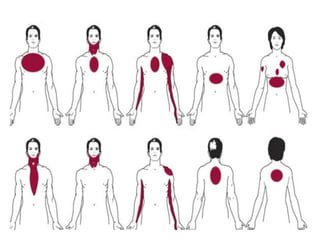
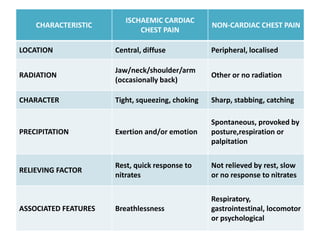
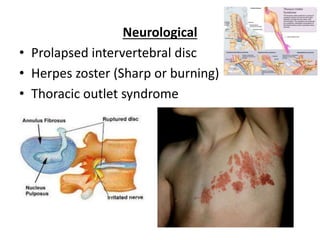
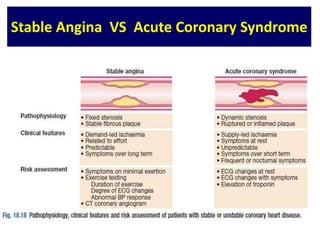
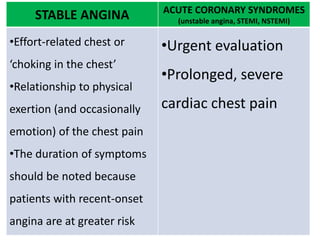
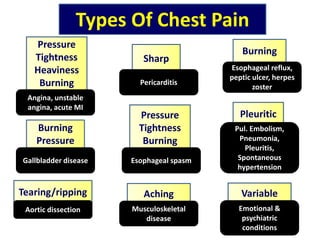
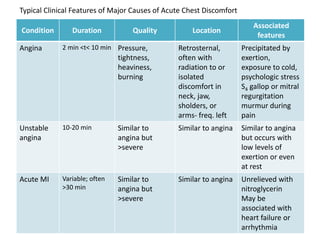
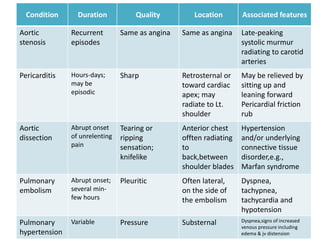
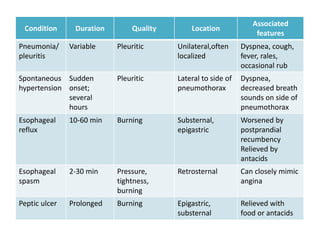
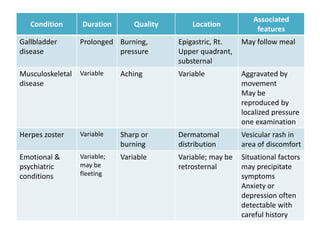
Chest pain can be cardiac or non-cardiac in origin. Cardiac causes include angina, myocardial infarction, and pericarditis while non-cardiac causes include pulmonary embolism, pneumonia, gallbladder disease, and musculoskeletal disorders. Characteristics of ischemic cardiac chest pain include a central, pressing or squeezing quality that radiates to the jaw/arm and is provoked by exertion. Differential diagnosis of chest pain requires evaluating characteristics like location, quality, duration and associated features to determine cardiac vs. non-cardiac etiology.































































![[Int. med] chest pain 3rd year class from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/zkh5x8lztsickjayhfry-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171705-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Int. med] chest pain 3rd year class](https://cdn.slidesharecdn.com/ss_thumbnails/int-150502144317-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)