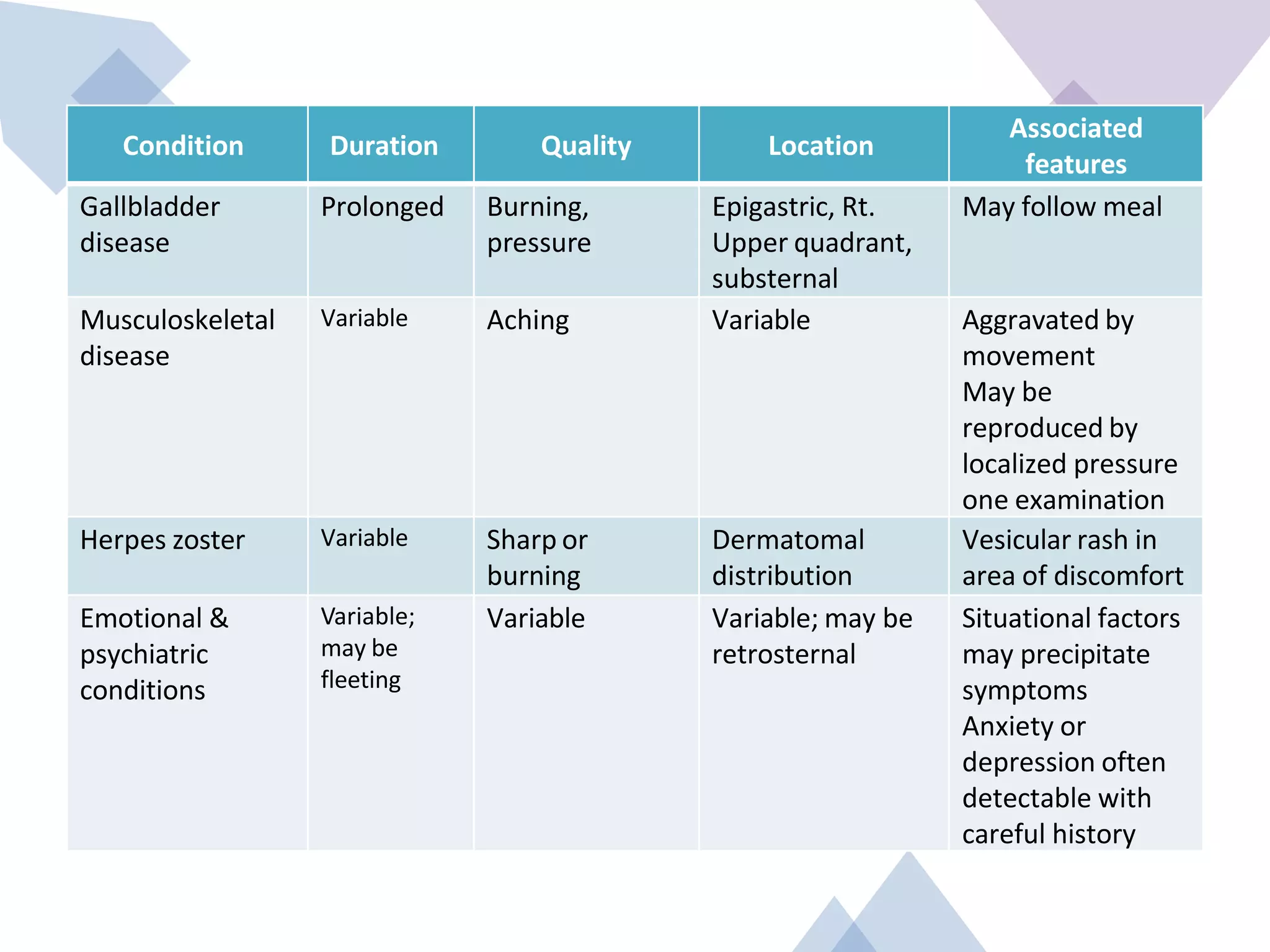
Chest pain can be cardiac or non-cardiac in origin. Cardiac causes include myocardial ischemia, angina, and acute coronary syndromes which present with characteristic dull, squeezing pain in the center of the chest that may radiate to the arms and is exacerbated by exertion. Non-cardiac causes include pulmonary embolism, pneumonia, gallbladder disease and musculoskeletal disorders which typically cause localized, sharp pains. A thorough history and physical exam is needed to differentiate cardiac from non-cardiac chest pain and determine appropriate treatment or need for further testing.















































































![[Int. med] chest pain 3rd year class from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/zkh5x8lztsickjayhfry-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171705-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Int. med] chest pain 3rd year class](https://cdn.slidesharecdn.com/ss_thumbnails/int-150502144317-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)










































