Downloaded 76 times

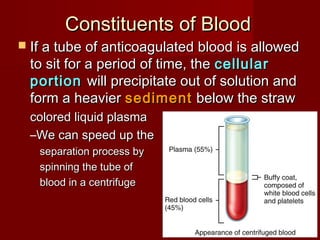
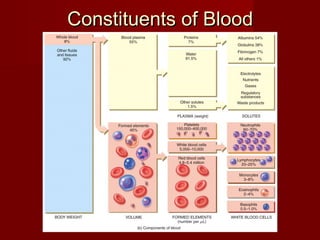
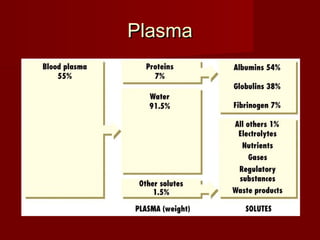
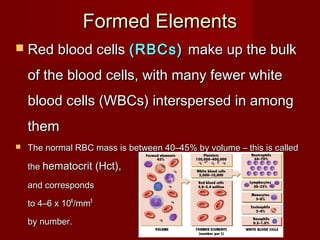
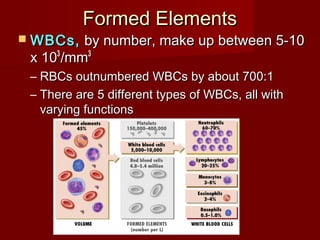
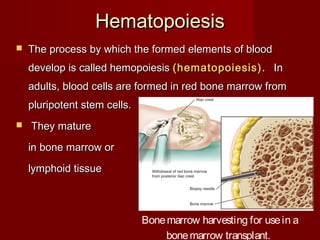
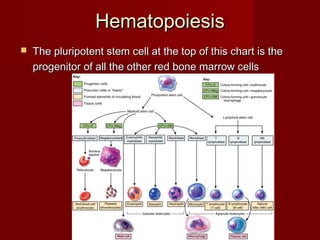
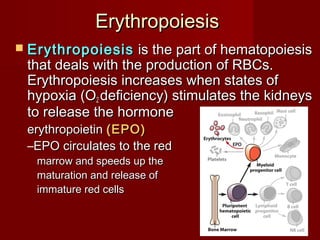
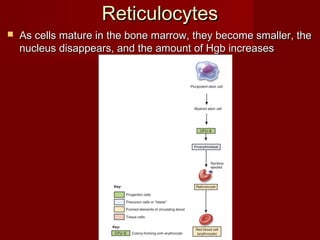
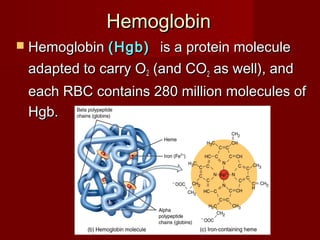

The document discusses the blood and its components. It states that blood contributes to homeostasis by transporting respiratory gases, nutrients, and hormones to and from cells. Blood also helps regulate pH and temperature, and provides protection through clotting and immune defenses. The document describes the constituents of blood including plasma and formed elements such as red blood cells, white blood cells, and platelets. It discusses hematopoiesis, the production of blood cells in the bone marrow, as well as abnormalities in erythropoiesis like anemia and polycythemia.




























































































![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)

