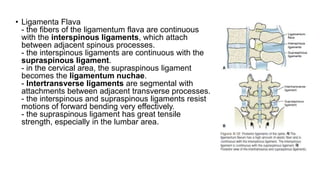
Downloaded 73 times
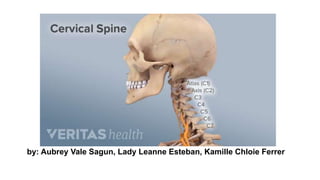
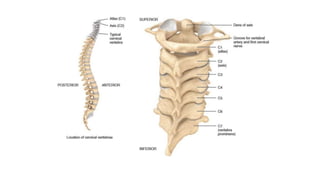
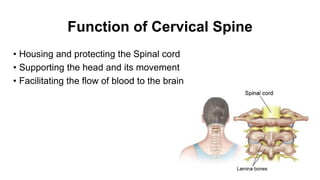
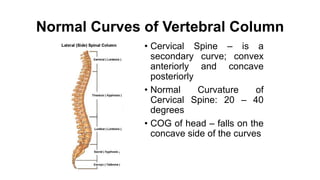
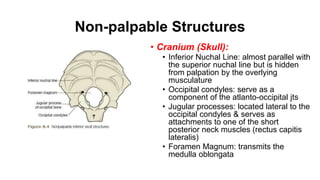
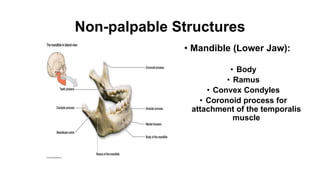
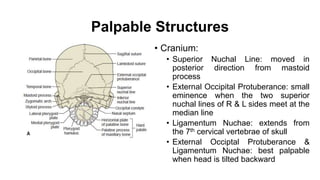
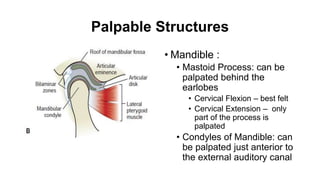
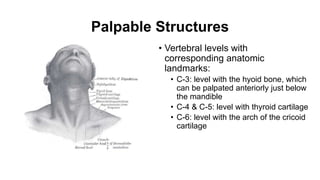

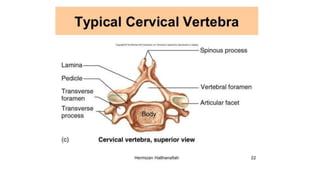
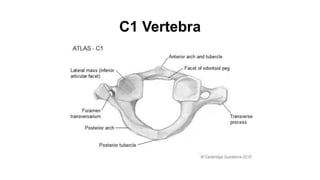
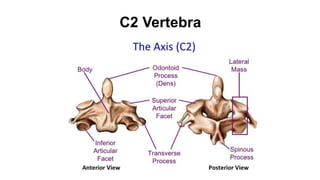
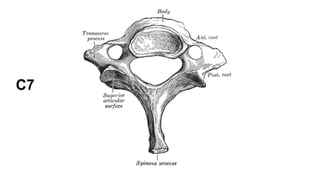
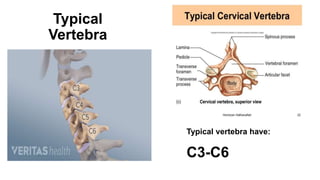
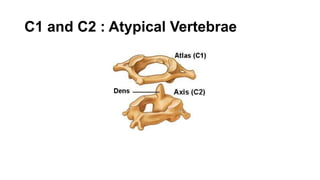
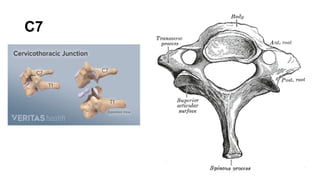
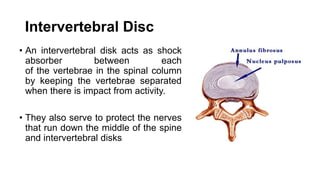
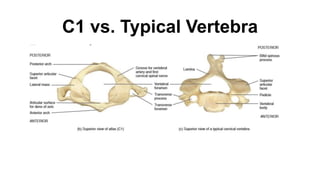
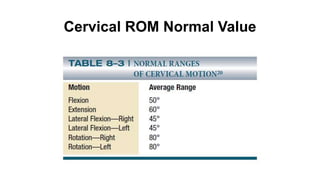
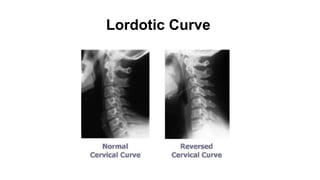

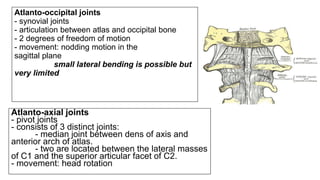
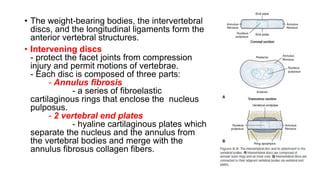
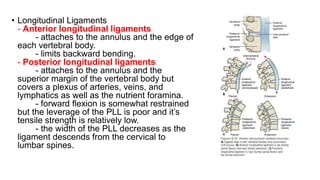

The cervical spine functions to house and protect the spinal cord, support the head and facilitate movement. It has a normal anterior curvature of 20-40 degrees. Non-palpable structures include the cranium, mandible, and vertebrae. Palpable structures are the superior nuchal line, external occipital protuberance, mastoid process, and vertebral levels C3-C6. Typical cervical vertebrae have transverse processes and spinous processes while C1-C2 are atypical. The intervertebral discs act as shock absorbers between vertebrae. Key joints are the atlanto-occipital and atlanto-axial, which allow nodding and rotation. Ligaments


































![MT-01 Anatomy and biomechanics of cervical spine-102024 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/mt-01anatomyandbiomechanicsofcervicalspine-102024autosaved-250827121120-fd4fe0b6-thumbnail.jpg?width=640&height=640&fit=bounds)














































