Downloaded 275 times

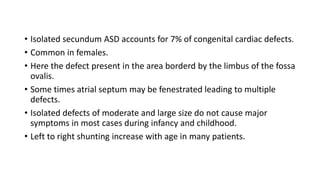
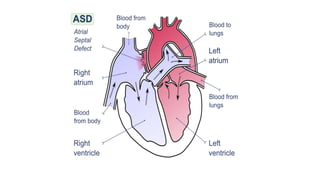

1. The atrial septum normally develops between the 4th and 8th weeks of gestation through the formation of the septum primum and secundum. 2. Abnormal development can result in several types of atrial septal defects (ASDs), the most common being a secundum ASD located in the area of the fossa ovalis. 3. Rarer types include sinus venosus defects (above or below the oval fossa), coronary sinus defects, and ostium primum defects located at the atrioventricular junction. Each has distinct developmental features and associations.


















































































