Download to read offline
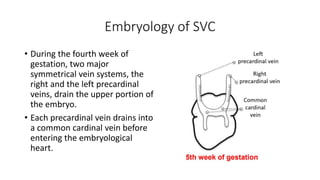
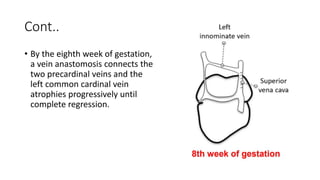
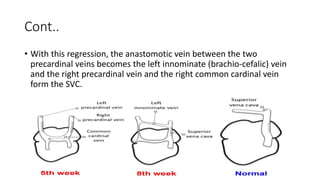

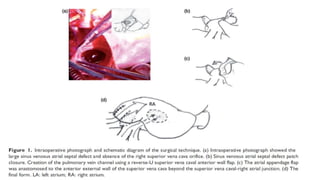



This document discusses a rare case of an anomalous right superior vena cava (RSVC) draining directly into the left atrium. The key points are: 1. Embryological development explains how the RSVC could anomalously connect to the left atrium. 2. A 34-year-old woman presented with hypoxemia and was found to have this rare condition. 3. Surgical correction was performed to reroute the RSVC into the right atrium, resolving the hypoxemia.












































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










