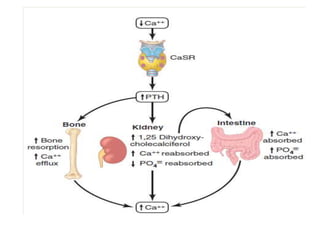
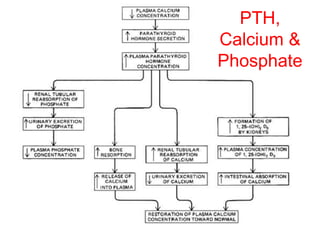
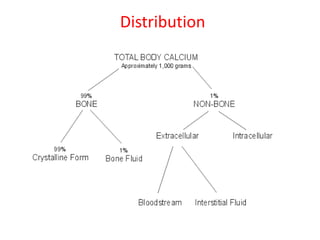
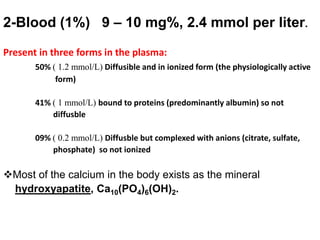
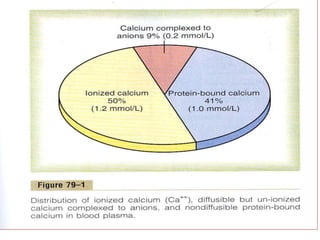
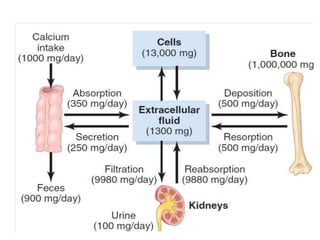
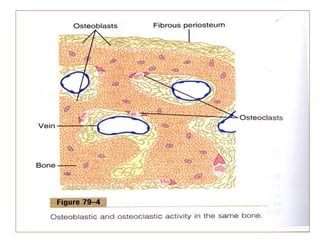
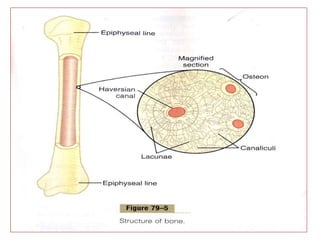
This document discusses calcium and phosphate metabolism and bone physiology. It begins by describing the functions and importance of calcium and phosphate in the body. The majority of calcium is stored in the bones, while calcium levels in blood and extracellular fluid are tightly regulated. Several hormones, including PTH, vitamin D, and calcitonin help regulate calcium levels. PTH and vitamin D work to increase calcium levels by promoting bone resorption and intestinal absorption, while calcitonin decreases calcium levels by inhibiting bone resorption. The kidneys also play an important role in calcium regulation through hormone-modulated reabsorption and excretion.

![Regulation of PTH
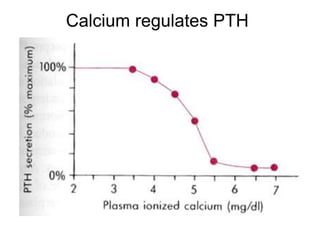
• The dominant regulator of PTH is plasma Ca2+.
• Secretion of PTH is inversely related to [Ca2+].
• Maximum secretion of PTH occurs at plasma
Ca2+ below 3.5 mg/dL.
• At Ca2+ above 5.5 mg/dL, PTH secretion is
maximally inhibited.](https://image.slidesharecdn.com/cametabolismandbonephysiology-200709090220/85/Ca-metabolism-and-bone-physiology-51-320.jpg)