Downloaded 163 times








![CALCIUM HOMEOSTASIS
Total Ca++
100 %
Protein bond
40 %
Ultrafilterable
60 %
Complexed to
anion
10 %
Ionized ca++
50 %
Body
content
Bone intracellular extracellular
Calcium 1300
gm
99% 1% 0.1%
▻Total plasma [Ca++] = 2.5mmol/L
▻Range is 2.1 to 2.6 mmol/L (8.8–10.4 mg/dL)
▻Very tightly controlled
▻Only free, ionized Ca2+ is biologically active.
▻Forms of Ca++ in the blood](https://image.slidesharecdn.com/bonephysiologyandcalciumhomeostasis-171002070050/75/Bone-physiology-and-calcium-homeostasis-21-2048.jpg)
![CALCIUM HOMEOSTASIS
Factors affecting calcium concentration:
▰ Changes in plasma protein concentration
Increased [protein] increased total [Ca2+]
▰ Changes in anion concentration
Increased [anion] increased fraction of Ca2+ that is complexed
decrease ionized [Ca2+]
▰ Acid base abnormality](https://image.slidesharecdn.com/bonephysiologyandcalciumhomeostasis-171002070050/75/Bone-physiology-and-calcium-homeostasis-22-2048.jpg)




![REFERENCES
▰ Linda S. Costanzo ,[2017] Physiology, 6th ed. by Elsevier, Inc. Richmond,
Virginia, USA.
▰ Solomon L., Warwick D. , Nayagam S.,[2010] Apley’s System of Orthopaedics
and Fractures, 9th ed. Hodder Arnold comp. ,London, UK.
▰ Fogelman I., Gnanasegaran G., [2012] Radionuclide and Hybrid Bone Imaging,
1st ed. Springer-Verlag Berlin Heidelberg, Berlin, Germany.
▰ John E. Hall Arthur C. Guyton, [2013] Textbook Of Medical Physiology, 13th ed.
By Mosby, An Imprint of Elsevier , Tennessee, USA.
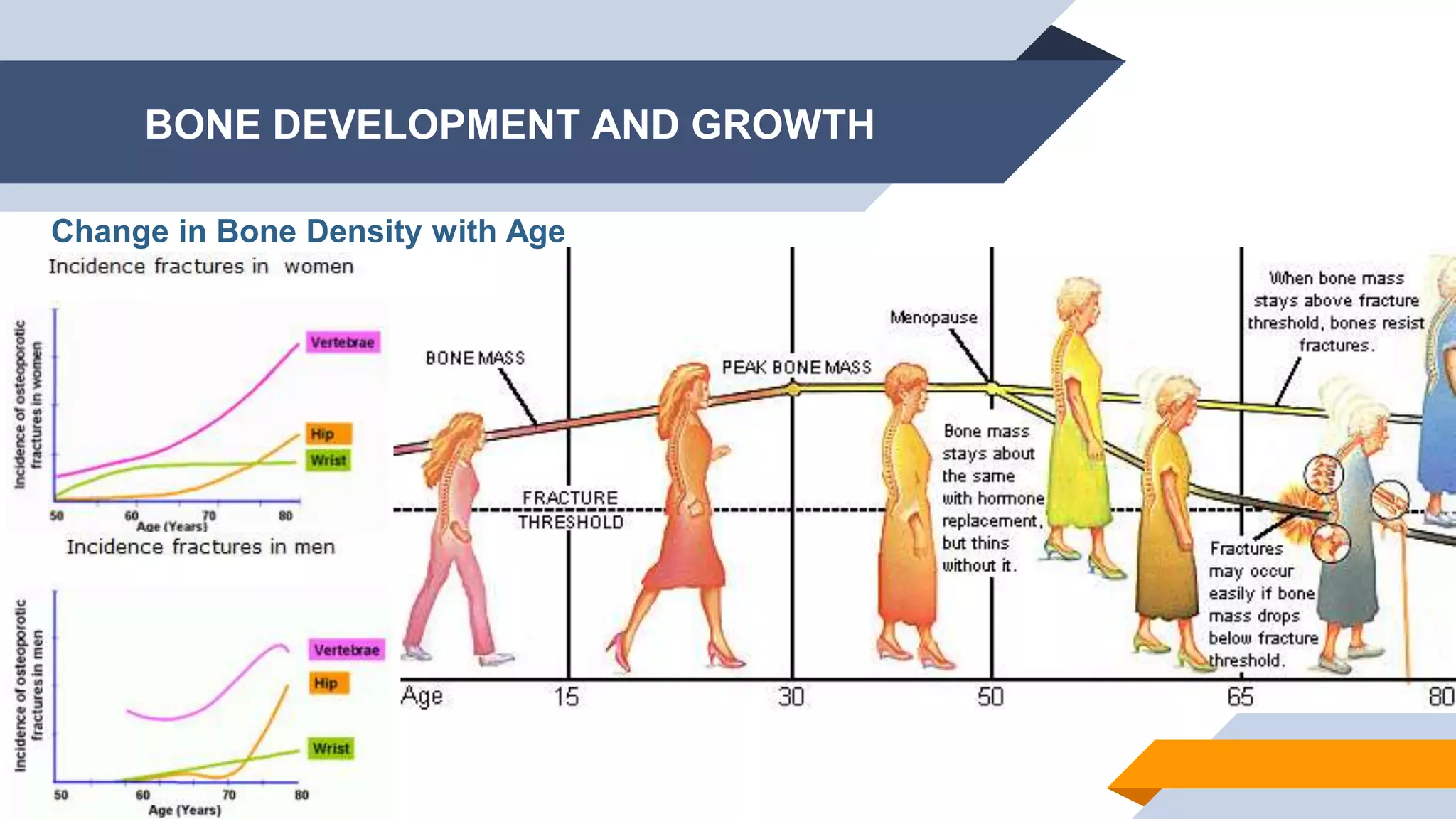
▰ Khosla S1, Riggs BL.[2005] Pathophysiology Of Age-related Bone Loss And
Osteoporosis, Endocrinol Metab Clin N Am 34 (2005) 1015–1030](https://image.slidesharecdn.com/bonephysiologyandcalciumhomeostasis-171002070050/75/Bone-physiology-and-calcium-homeostasis-31-2048.jpg)


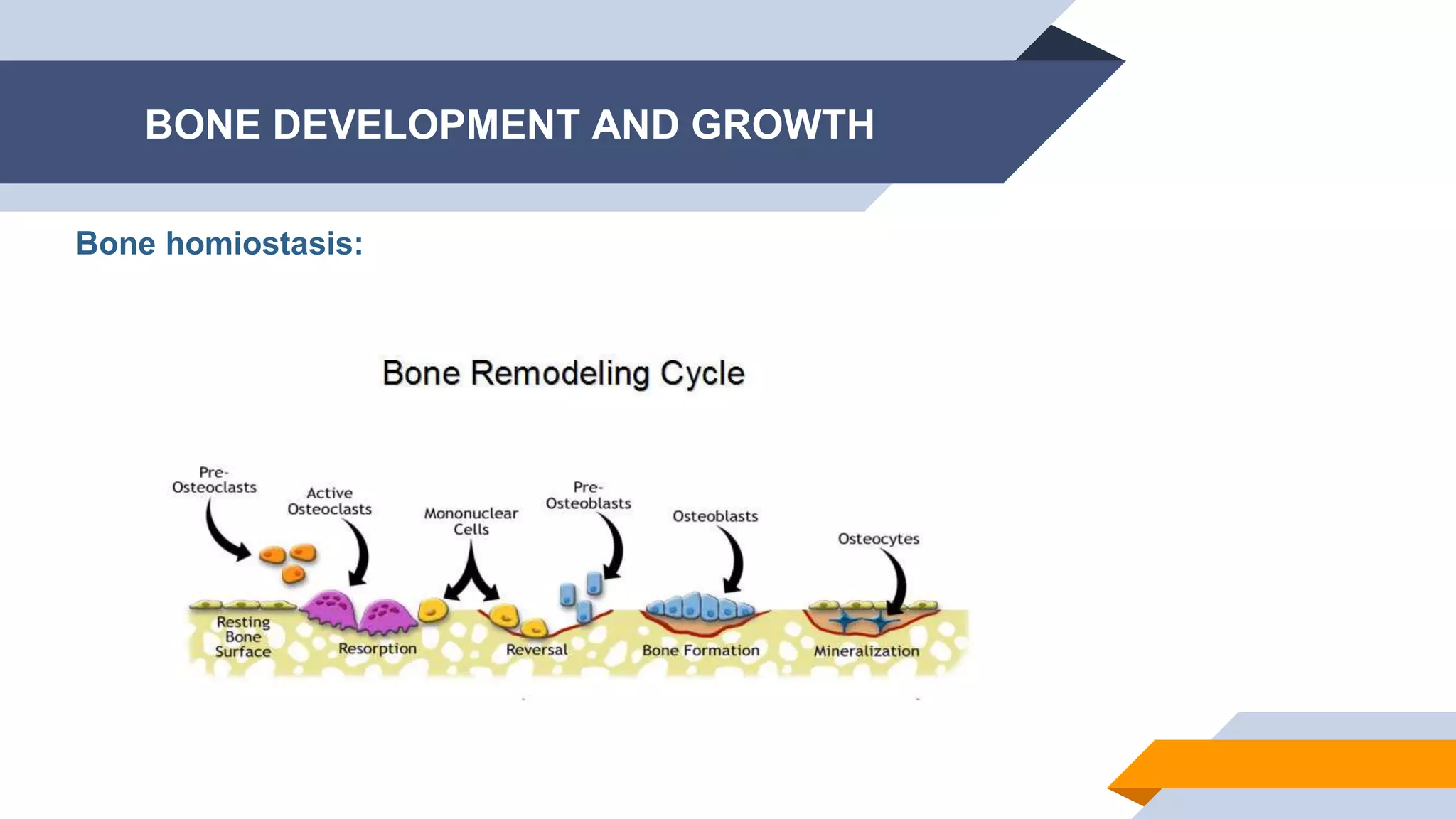
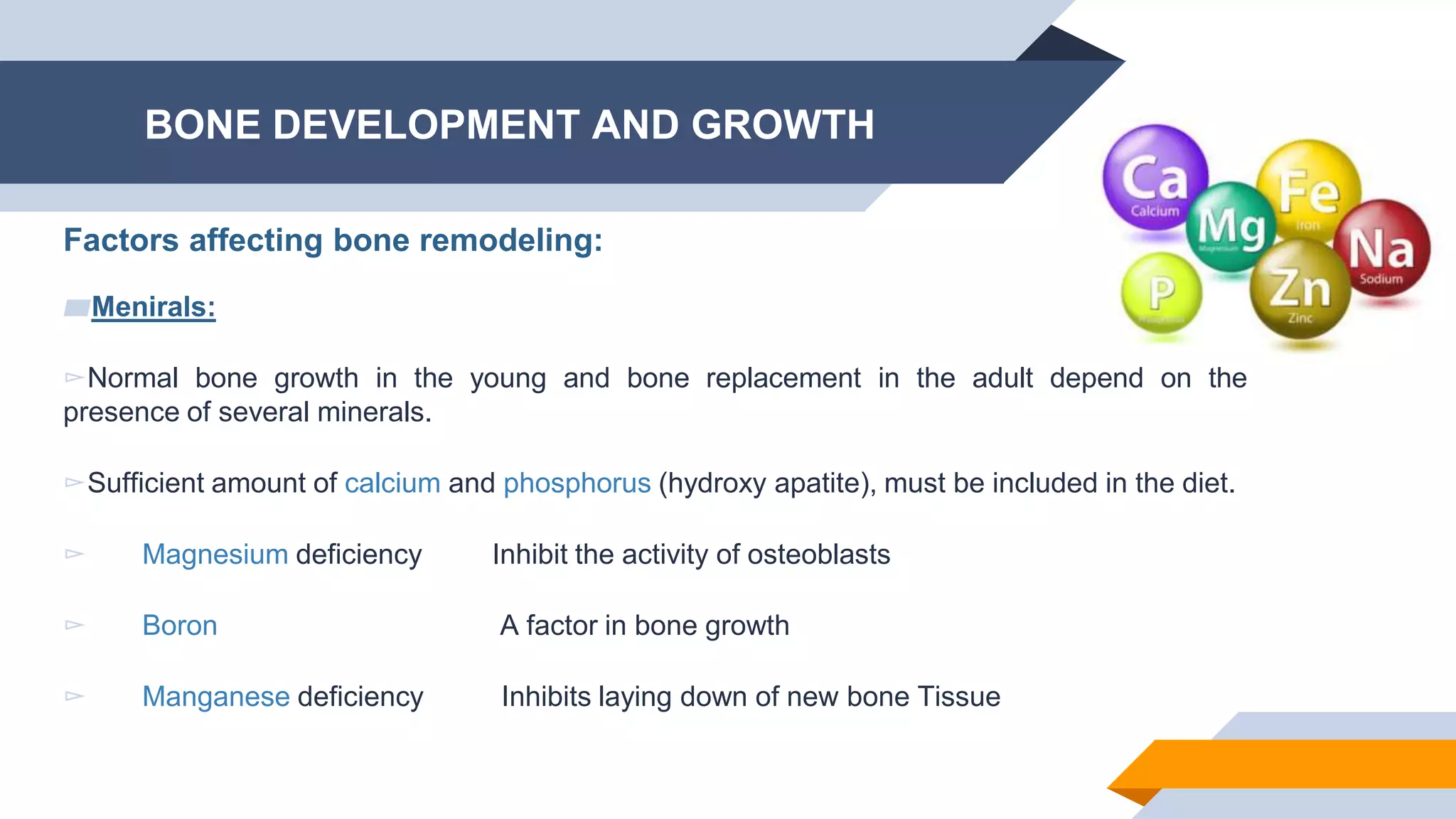
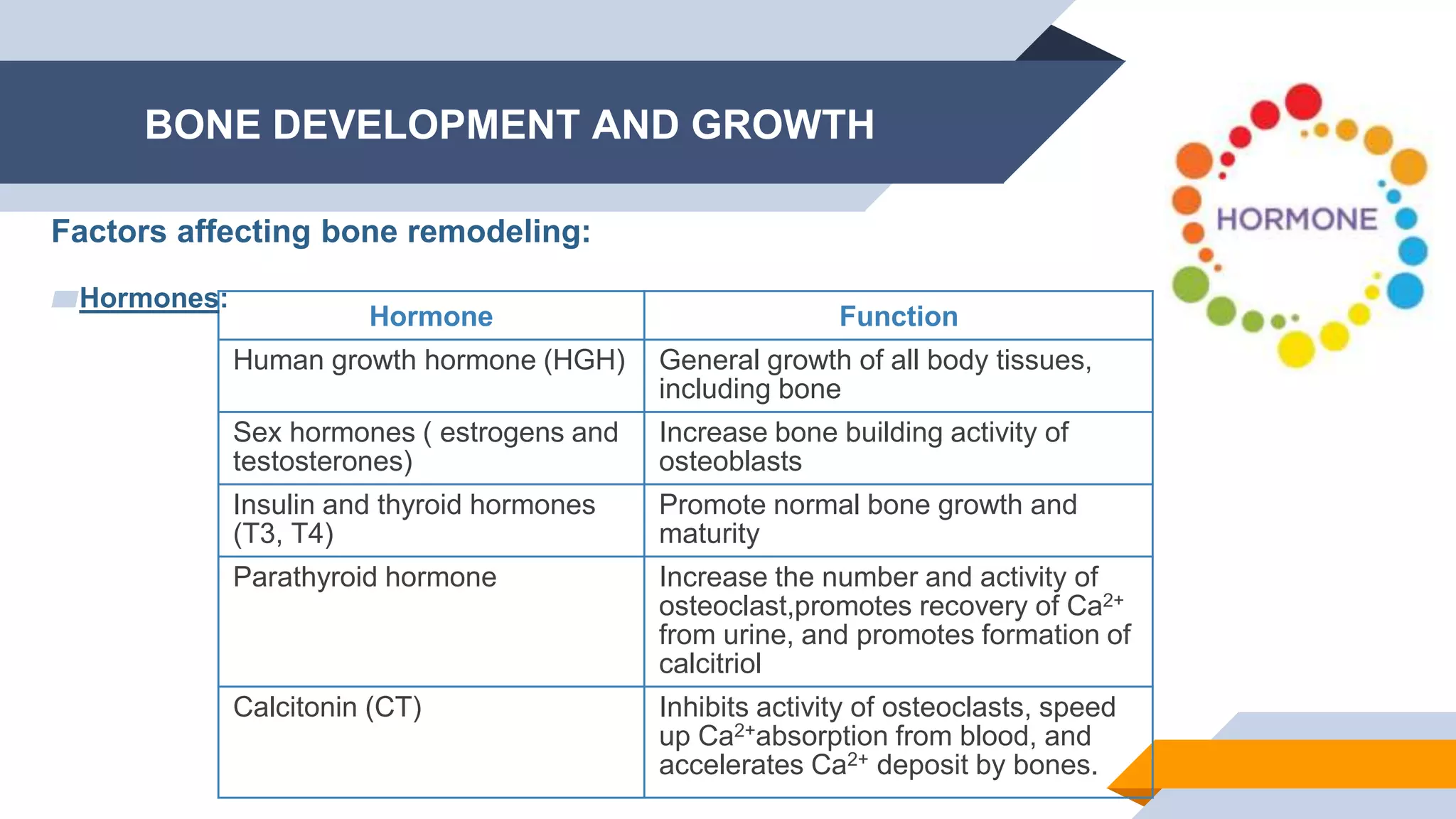
The document discusses bone physiology and calcium homeostasis, highlighting the composition, structure, and growth of bone, as well as factors that influence bone development and remodeling. It explains the roles of different cell types like osteoblasts and osteoclasts, the process of ossification, and the hormonal regulation of calcium levels. Additionally, it emphasizes the importance of minerals and vitamins in bone health and their functions in the body.

















![Osteomalacia 2nd-150704155942-lva1-app6892 [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/osteomalacia-2nd-150704155942-lva1-app6892autosaved-200520081743-thumbnail.jpg?width=640&height=640&fit=bounds)




































































