Downloaded 41 times
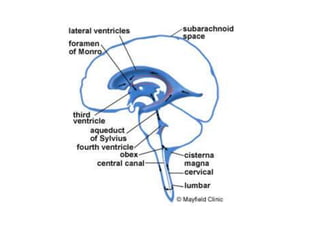
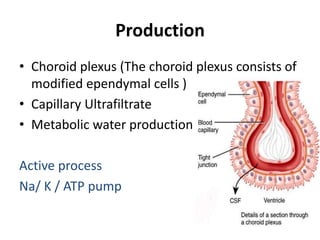
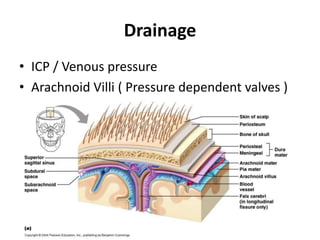


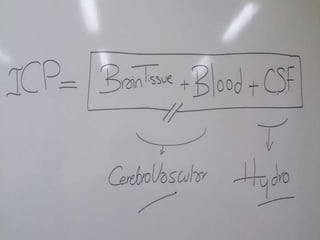
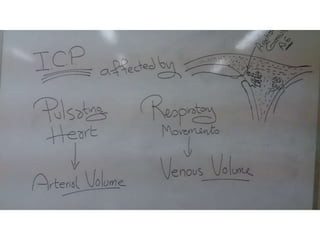
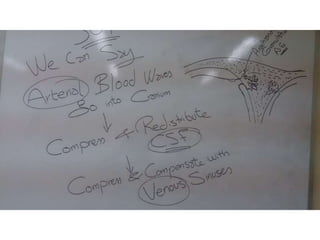
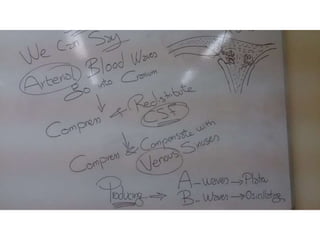

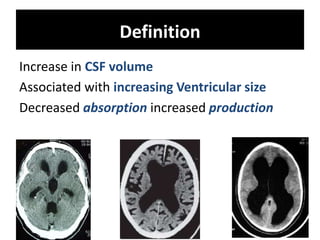


This document discusses cerebrospinal fluid (CSF) dynamics, including CSF production, drainage, composition, and pressure. Key points include: - CSF is produced by the choroid plexus at a rate of 0.3-0.4 ml/min and is absorbed through the arachnoid villi and dural sinusoids. - Normal CSF pressure in adults is 4.5-13.5 mmHg. - Infusion tests can assess CSF system dynamics by measuring parameters like conductance and compliance. - Understanding CSF dynamics helps research hydrocephalus and could aid in deciding treatment like shunt surgery.























































































