Downloaded 72 times
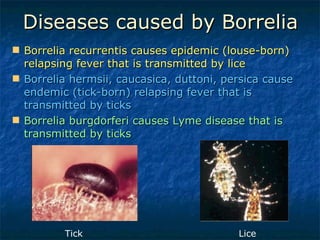

1. Curviform bacteria like Campylobacter, Helicobacter, and Vibrio can cause diseases in humans. 2. Campylobacter causes enterocolitis and diarrhea. Helicobacter pylori causes gastritis and peptic ulcers. 3. Spirochetes are spiral-shaped bacteria including Treponema, Borrelia, and Leptospira. Some are human pathogens that cause diseases like syphilis, Lyme disease, and relapsing fever.


















































































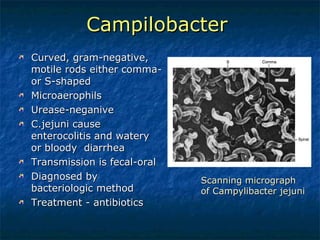
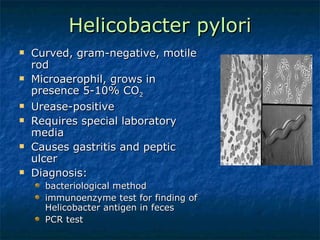
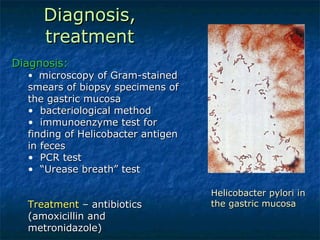
![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)













