Downloaded 985 times




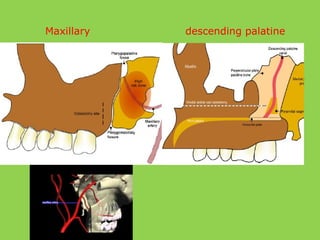
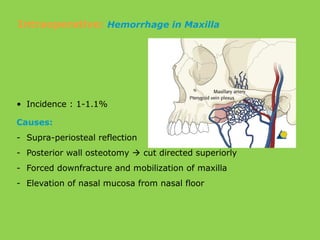
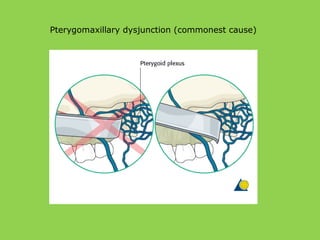
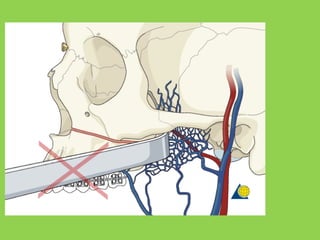
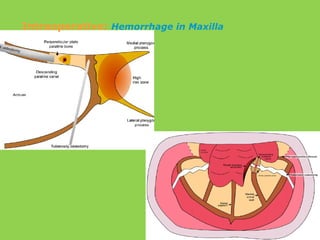

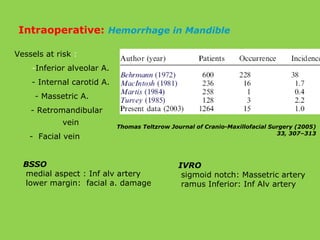
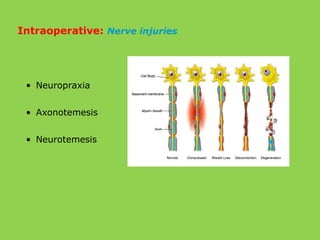

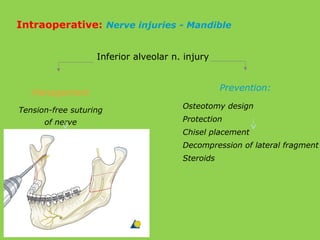

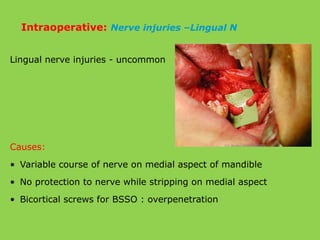
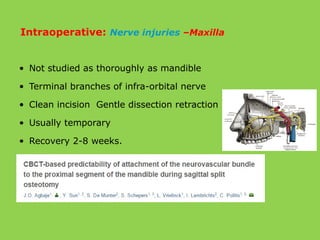
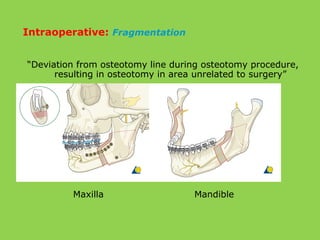
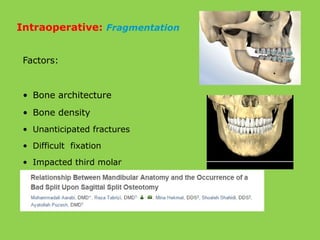

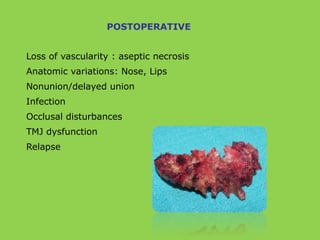
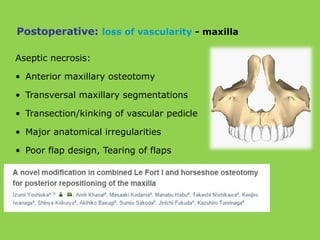
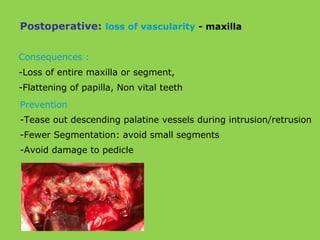
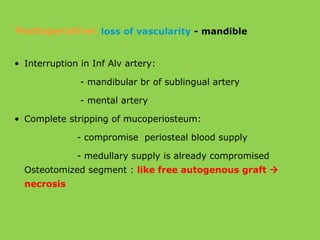
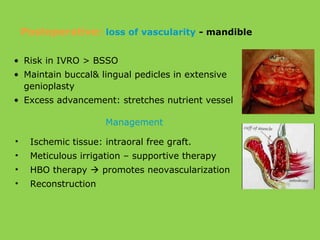
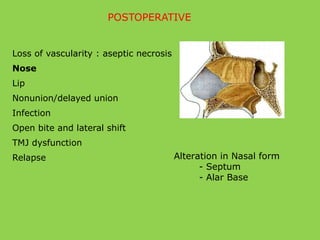
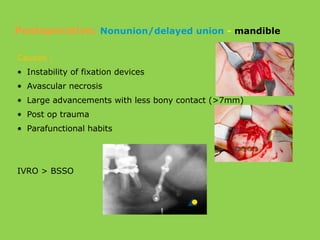


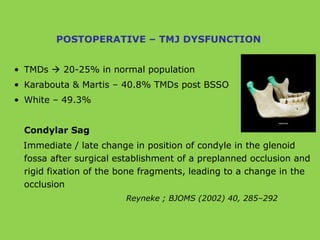
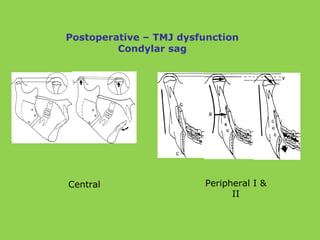
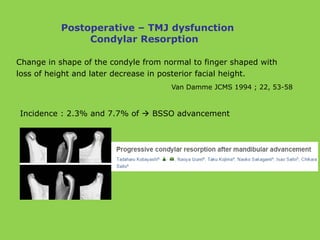



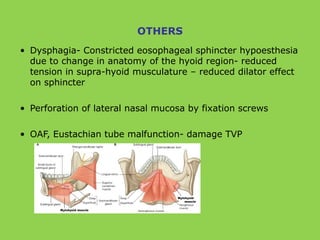



This document discusses various complications that can occur with orthognathic surgery, including: - Common intraoperative complications are nerve injuries, most often to the inferior alveolar nerve during mandibular surgery, and hemorrhage, usually from the maxillary arteries. - Frequent postoperative issues involve neurosensory deficits, nonunion or delayed bone healing, and infections, which have been reported in up to 9.7% of patients. - Other risks include loss of vascularity leading to aseptic necrosis of the maxilla or mandible, nasal deformities, malocclusion, and TMJ dysfunction. Careful planning and technique aim to minimize complications while pursuing the benefits of orthognathic

































































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)




