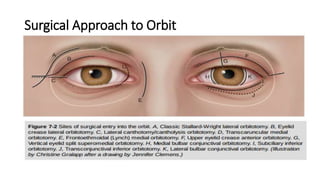
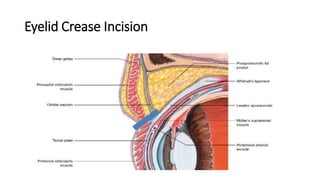
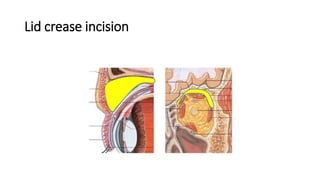
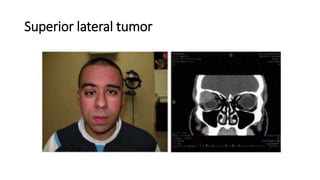
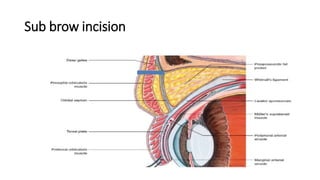
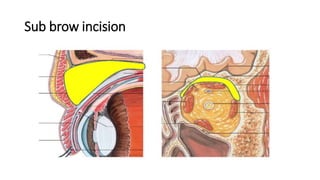
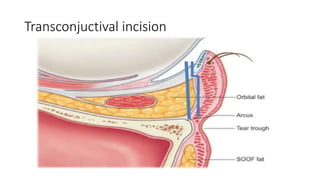
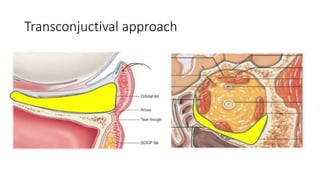
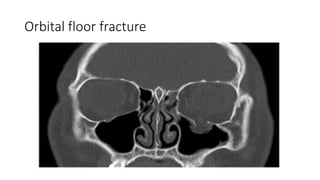
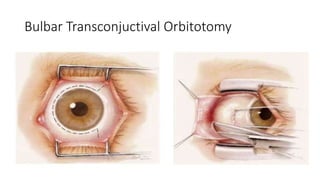
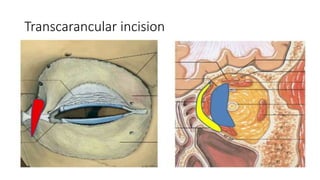
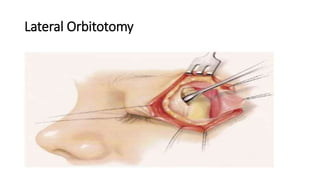
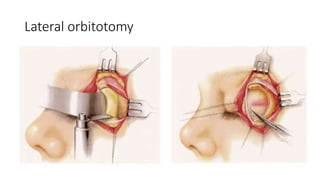
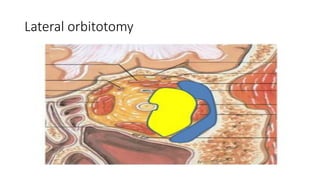
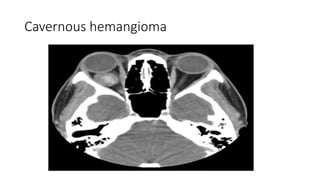
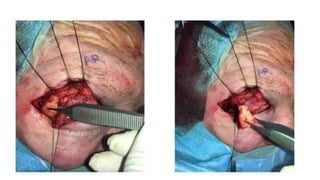
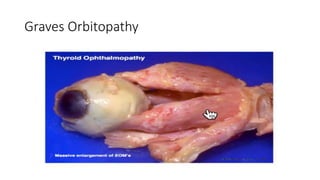
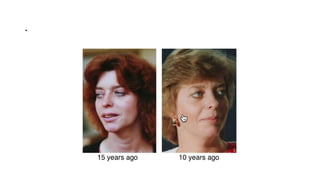
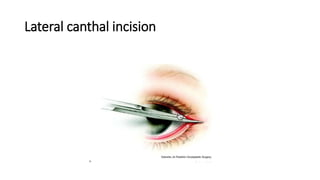
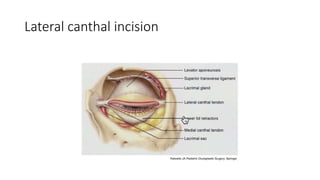
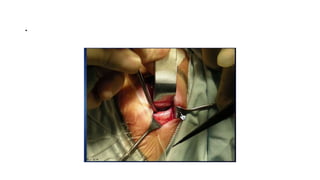
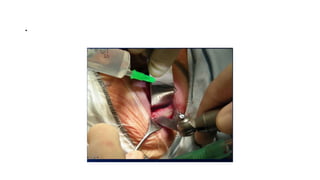
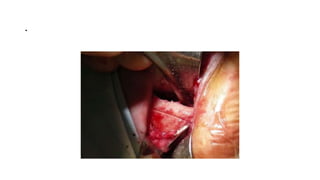
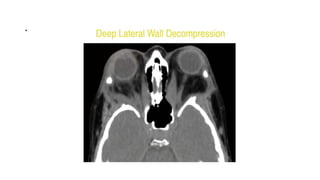
This document summarizes a presentation on orbital surgery. It discusses various surgical approaches to the orbit including lid crease incisions, lateral orbitotomies, and endoscopic decompression. It also covers orbital decompression techniques like superior, medial, inferior and lateral decompression to treat conditions like Graves' orbitopathy. Potential complications of orbital surgery are discussed such as diplopia, optic neuropathy, and hypoesthesia, as well as techniques to avoid complications by careful patient evaluation, approach selection, exposure and hemostasis.