Downloaded 432 times
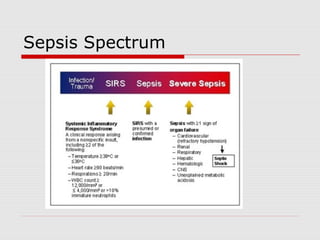
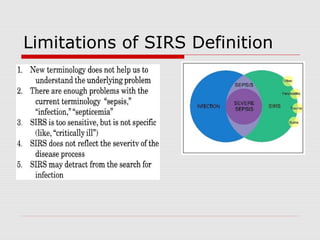
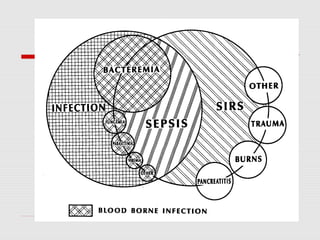
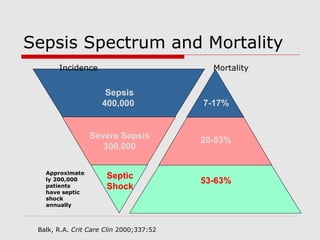
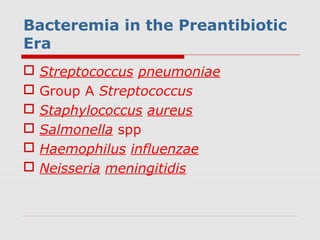
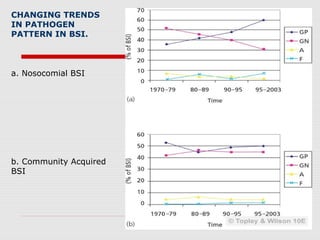

This document discusses bloodstream infections, including definitions, types, causes, and trends. It defines terms like bacteremia, sepsis, and community-acquired versus nosocomial bloodstream infections. Primary bloodstream infections often originate from intravascular devices, while secondary infections usually stem from a focus elsewhere in the body. Common pathogens have changed over time and vary based on healthcare or community setting. Prompt diagnosis and treatment are important given the high mortality rates associated with severe sepsis and septic shock.