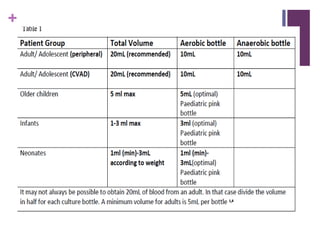
The document provides guidelines for collecting blood cultures to detect bloodstream infections. It states that blood cultures should only be collected when there is a clinical indication of sepsis based on symptoms such as fever, tachycardia, or confusion. It emphasizes the importance of following proper technique to minimize contamination, including cleaning the skin with chlorhexidine, collecting cultures through a newly inserted needle before other blood draws, and clearly labelling the sample source. The document also provides step-by-step instructions for collecting both peripheral blood cultures and cultures from central venous access devices.












































![BLOOD CULTURE; MANUAL PROCEDURE [power point]](https://cdn.slidesharecdn.com/ss_thumbnails/bloodculturemanualprocedure-250329002331-f87e46f6-thumbnail.jpg?width=640&height=640&fit=bounds)




























