Downloaded 350 times














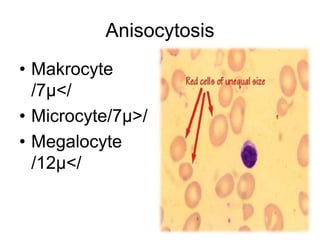






















































The document discusses various blood disorders including changes in blood volume, anemias, and other conditions that affect the cellular components of blood. It describes how hypovolemia, hypervolemia, and normovolemia impact blood volume. Specific types of anemia are outlined such as iron-deficiency anemia, megaloblastic anemias, and aplastic anemia. Abnormal red blood cell morphologies associated with different anemias are also reviewed. Other conditions examined include polycythemia, leukopenia, leukocytosis, neutrophil shift, leukemia, and lymphoma.











































































































