INTRODUCTION
Anemia is diagnosedas any condition in which there
is a decreased number of circulating red blood cells.
Conditions where our body does not produce enough
healthy red blood cells, destroys too many red blood
cells, or loses circulating red blood cells can all lead
to anemia.
Anaemia, as per is not a specific disease state but a
sign of underlying disorder.
3.
Anaemia is acondition in which the number of red blood cells or
the hemoglobin concentration within them is lower than normal
4.5 – 6.5 million
4.
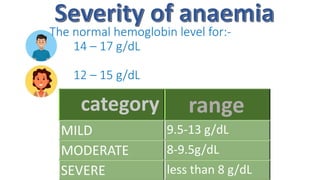
The normal hemoglobinlevel for:-
14 – 17 g/dL
12 – 15 g/dL
category range
MILD 9.5-13 g/dL
MODERATE 8-9.5g/dL
SEVERE less than 8 g/dL
4
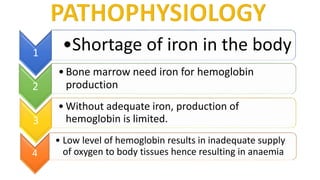
• Low levelof hemoglobin results in inadequate supply
of oxygen to body tissues hence resulting in anaemia
1
•Shortage of iron in the body
2
•Bone marrow need iron for hemoglobin
production
3
• Without adequate iron, production of
hemoglobin is limited.
7.
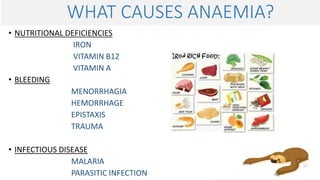
WHAT CAUSES ANAEMIA?
•NUTRITIONAL DEFICIENCIES
IRON
VITAMIN B12
VITAMIN A
• BLEEDING
MENORRHAGIA
HEMORRHAGE
EPISTAXIS
TRAUMA
• INFECTIOUS DISEASE
MALARIA
PARASITIC INFECTION
8.
•Diet lacking incertain elements such as iron and
vitamins
•Intestinal disorders
•Menstruation
•Pregnancy
•Age
•Chronic conditions
9.
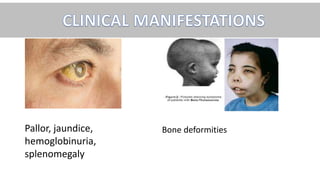
• Fatigue /weaknessand pallor, headache, due to hypoxia
• Dyspnea, hypotension, tachycardia, systolic murmur
• Bone pain
• Jaundice in hemolytic anaemia
• Splenomegaly and angina pectoris
10.
This typically resultsdue to inadequate intake of dietary iron .
Common cause in men and post menopausal women is bleeding, in pre
menopausal women is menorrhagia and pregnancy with inadequate iron
supplements. Other causes may include mal absorption often seen after
gastrostomy/ celiac disease.
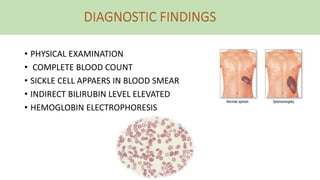
• COMPLETE BLOODCOUNT
MOST RELIABLE DIAGNOSTIC FINDING IS FERRITIN AND HEMOGLOBIN VALUES.
• FERRITIN BLOOD TEST
• BONE MARROW ASPIRATE
13.
• ORAL REPLACEMENT
-Ferrous sulphate
- Ferrous gluconate
- Ferrous fumarate
• PARENTAL REPLACEMENT
- Iron dextran
- Iron sodium gluconate
- Iron sucrose complex
14.
NURSING INTERVENTIONS
• Monitorvital signs for tachycardia/ tachypnea
• Monitor for reaction to parental therapy
• Promote iron intake
• Educate patient for
-sources of dietary iron and vitamin C intake
-restrictions and way of taking dose
-side effects
15.
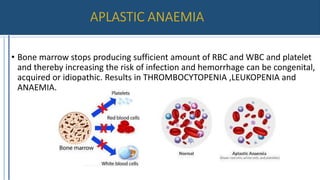
• Bone marrowstops producing sufficient amount of RBC and WBC and platelet
and thereby increasing the risk of infection and hemorrhage can be congenital,
acquired or idiopathic. Results in THROMBOCYTOPENIA ,LEUKOPENIA and
ANAEMIA.
16.
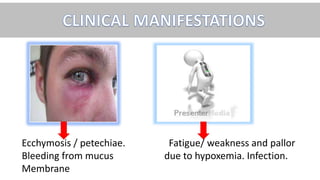
Ecchymosis / petechiae.Fatigue/ weakness and pallor
Bleeding from mucus due to hypoxemia. Infection.
Membrane
MEDICAL MANAGEMENT
• Administerhematopoietic factor
- Epoetin Alfa by SC/IV
• Administer human granulocyte colony stimulating factor
- filgrastim by SC/IV
-sargramostim by IV infusion
• Packed RBC transfusion when Anaemia is symptomatic
• Platelet transfusion for severe bleeding
• Administer immunosuppressive drugs, antithymocyte, globulin and corticosteroids.
• BONE MARROW TRANSPLANT:- replacing non functional stem cells
19.
NURSING INTERVENSTIONS
• Monitorvitals for changes
• Report intake and output of fluids
• Protect patient from falls
• Avoid IM injections due to altered clotting ability
• Explain the patient
-No aspirin due to platelet aggregation
-Plan to take rest periods during activities
-Only use electric razor to decrease risk of bleeding
-Call physician/nurse for signs of bleeding
20.
• Anaemia causedby deficiency of vitamin B12 or folic acid.
RBC produced are abnormally large and may occur due to body’s
inability to absorb vitamin B12.
Typical onset is between 40-60years
21.
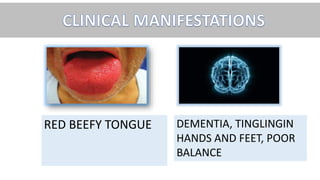
RED BEEFY TONGUEDEMENTIA, TINGLINGIN
HANDS AND FEET, POOR
BALANCE
NURSING INTERVENSTIONS
• Monitorvitals
• Manage fluid overload
• Monitor regular blood transfusion
• Urine color orange
• During blood transfusion iron
supplements should be restricted.
35.
NURSING DIAGNOSIS
• Activityintolerance related to fatigue
• Imbalanced nutrition less than body
requirements related to inadequate intake of
essential nutrients
• Insufficient tissue perfusion related to
inadequate blood volume
Condition of reducedRBC is known as Anaemia.
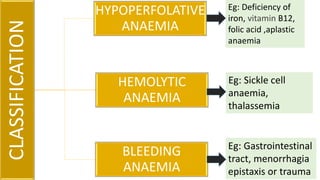
•3 classifications : hemolytic, hypo-proliferative, bleeding
• Risk factors : age, pregnancy, menstruation, intestinal
disorders etc.
• Clinical manifestations : fatigue, pallor,
dyspnea, splenomegaly, jaundice, tachycardia, etc.
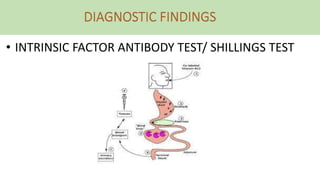
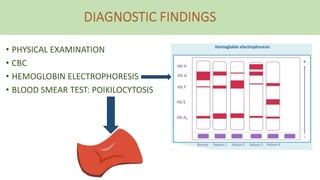
•Diagnosis : History, physical examination, CBC,
bone marrow aspirate, shillings test,
hemoglobin electrophoresis.
44.
Polycythaemia is overproduction of blood cells.
• Clinical manifestations: plethora, hypertension, severe
itching, headache, blurred vision, tinnitus, thrombosis
leading to tissue hypoxia.
• Diagnostic findings: CBC, bone marrow biopsy
• Management: phlebotomy, antihistamines,
anticoagulants, allopurinol etc.
45.
PLETHORA IS ACLINICAL MANIFESTATION OF
1. SICKLE CELL ANAEMIA
2. POLYCYTHAEMIA
3. THALASSEMIA
4. MEGALOBLASTIC ANAEMIA
46.
MEGALOBLASTIC ANAEMIA ISDEFICIENCY OF
1. IRON
2. VITAMIN C
3. VITAMIN B12 AND FOLIC ACID
4. VITAMIN A
47.
ANOTHER TERM FORMEGALOBLASTIC ANAEMIA
1. APLASTIC ANAEMIA
2. PERNICIOUS ANAEMIA
3. THALASSEMIA
4. SICKLE CELL ANAEMIA
48.
TRUE / FALSE
1.ANTACIDS AND DAIRY PRODUCTS SHOULD BE TAKEN WITH IRON
SUPPLEMENTS IN IRON DEFICIENCY ANAEMIA.
2. INSUFFICIENT INTAKE OF VITAMIN C CAN CAUSE MALABSORPTION
OF IRON IN BODY.
3. PHLEBOTOMY IS INDICATED IN POLYCYTHAEMIA.
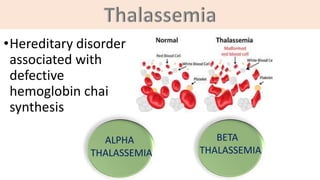
4. THALASSEMIA FALLS UNDER THE CLASSIFICATION OF
HYPOPERFOLATIVE ANAEMIA.
5. ALPHA THALASSEMIA IS THE SEVERE FORM OF
THALASSEMIA.
6. ALLOPURINOL LOWERS URIC ACID LEVELS
49.
NOT A DIAGNOSTICTEST FOR POLYCYTHAEMIA
1. CBC
2. BONE MARROW BIOPSY
3. HEMOGLOBIN ELECTROPHORESIS
4. LEVELS OF VITAMIN B12

































![BLOOD_DISORDERS-2[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/blooddisorders-21-230610142333-f4472c75-thumbnail.jpg?width=640&height=640&fit=bounds)



















![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

















