Downloaded 207 times
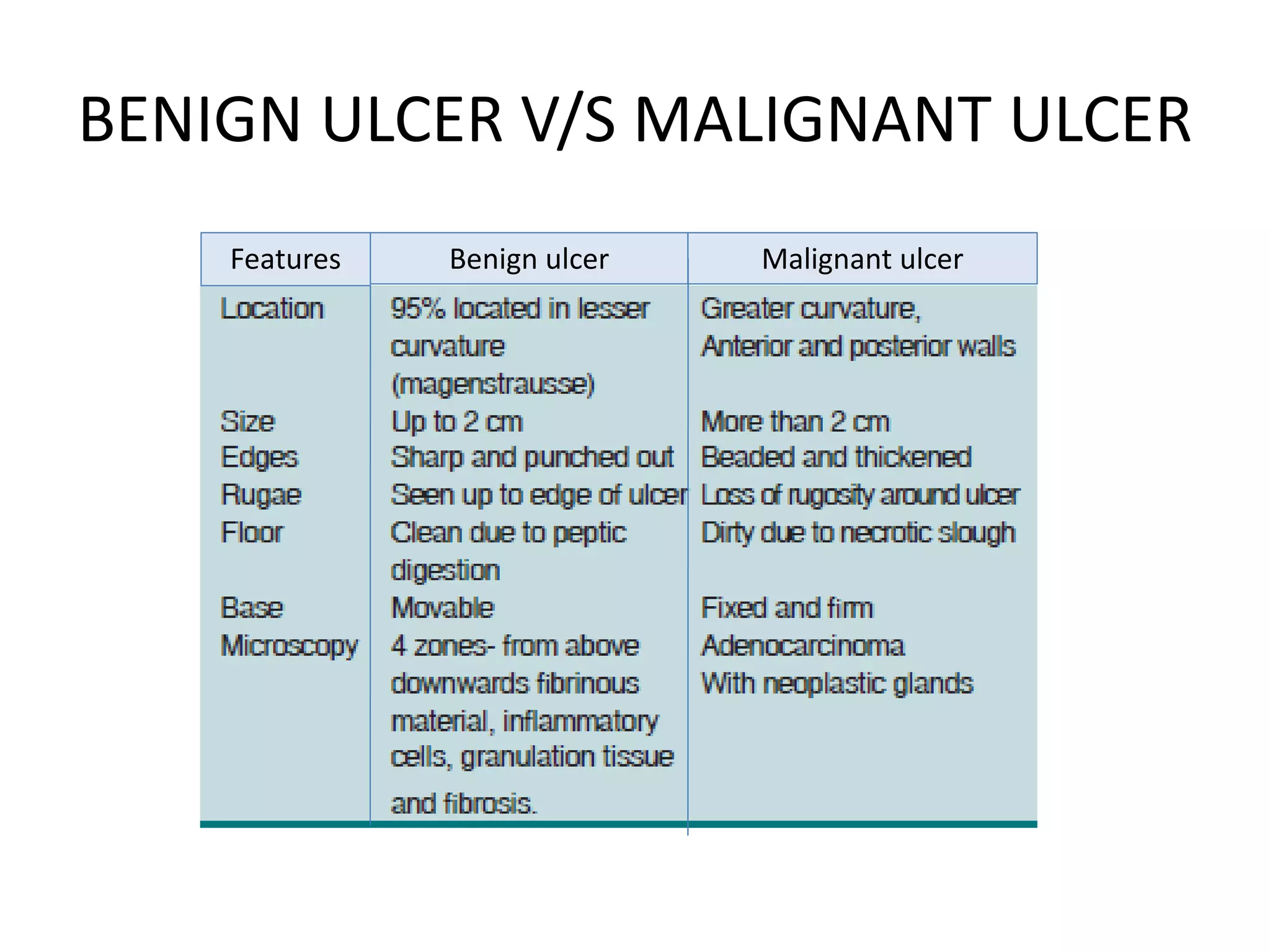
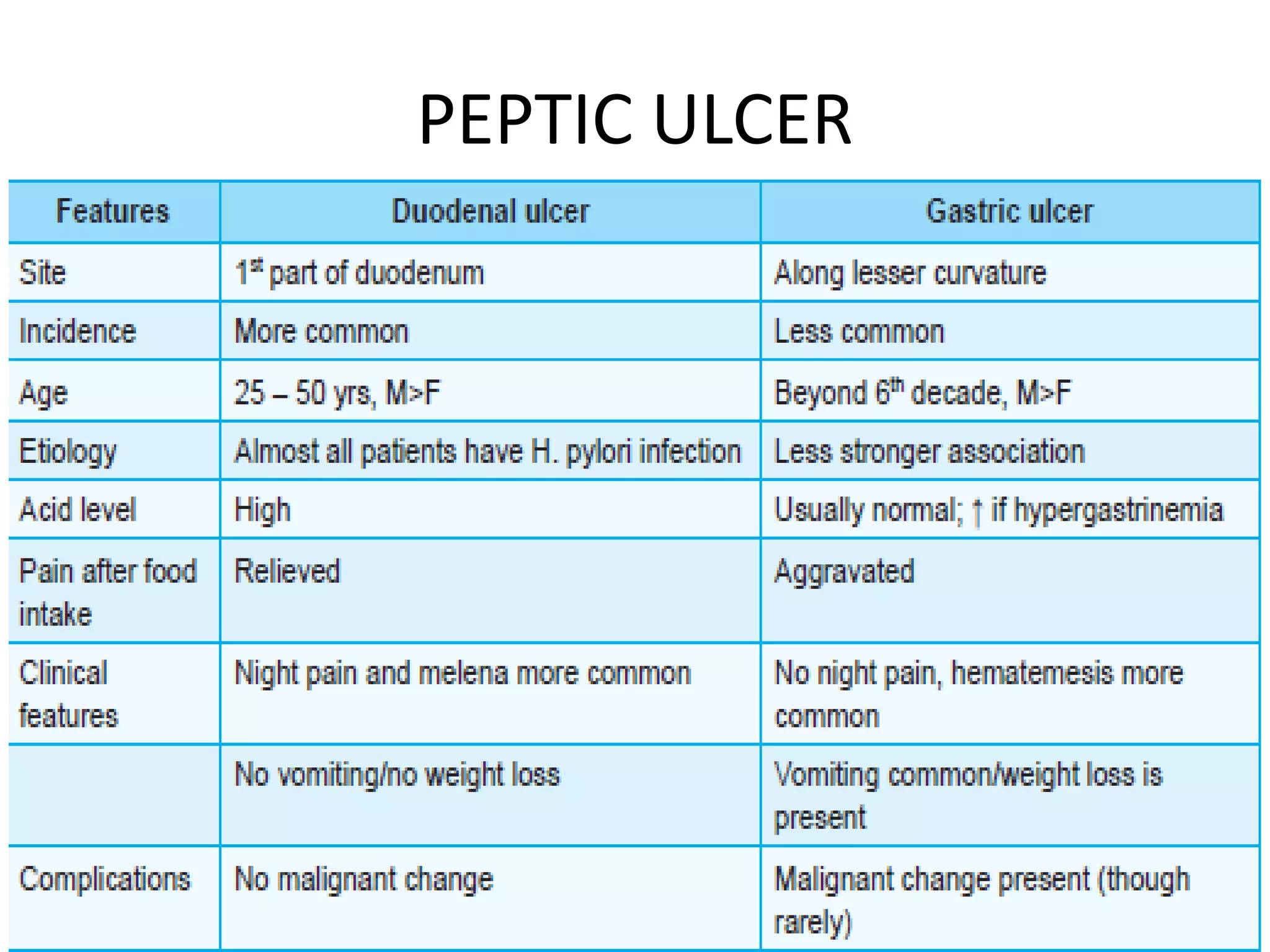

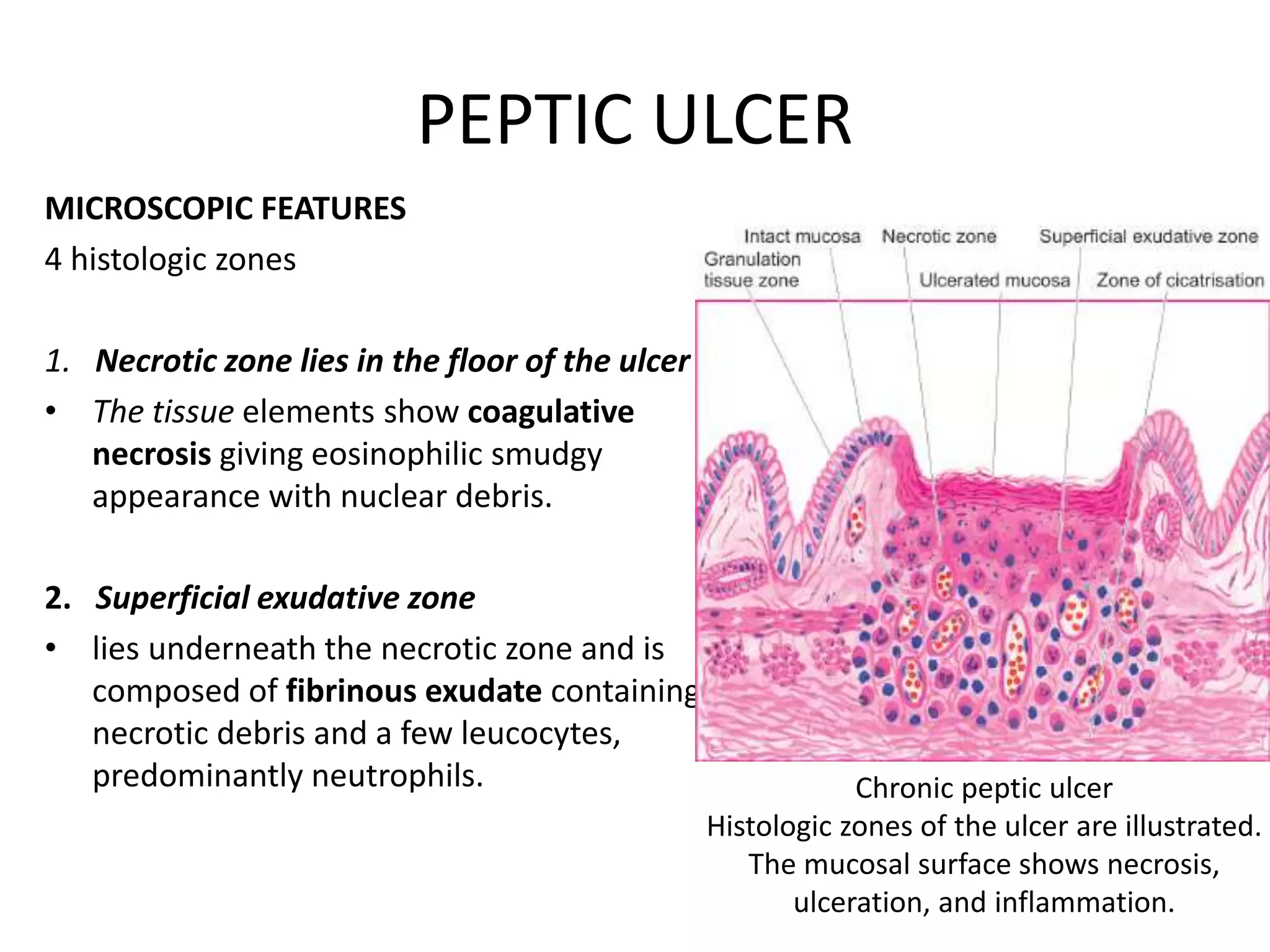
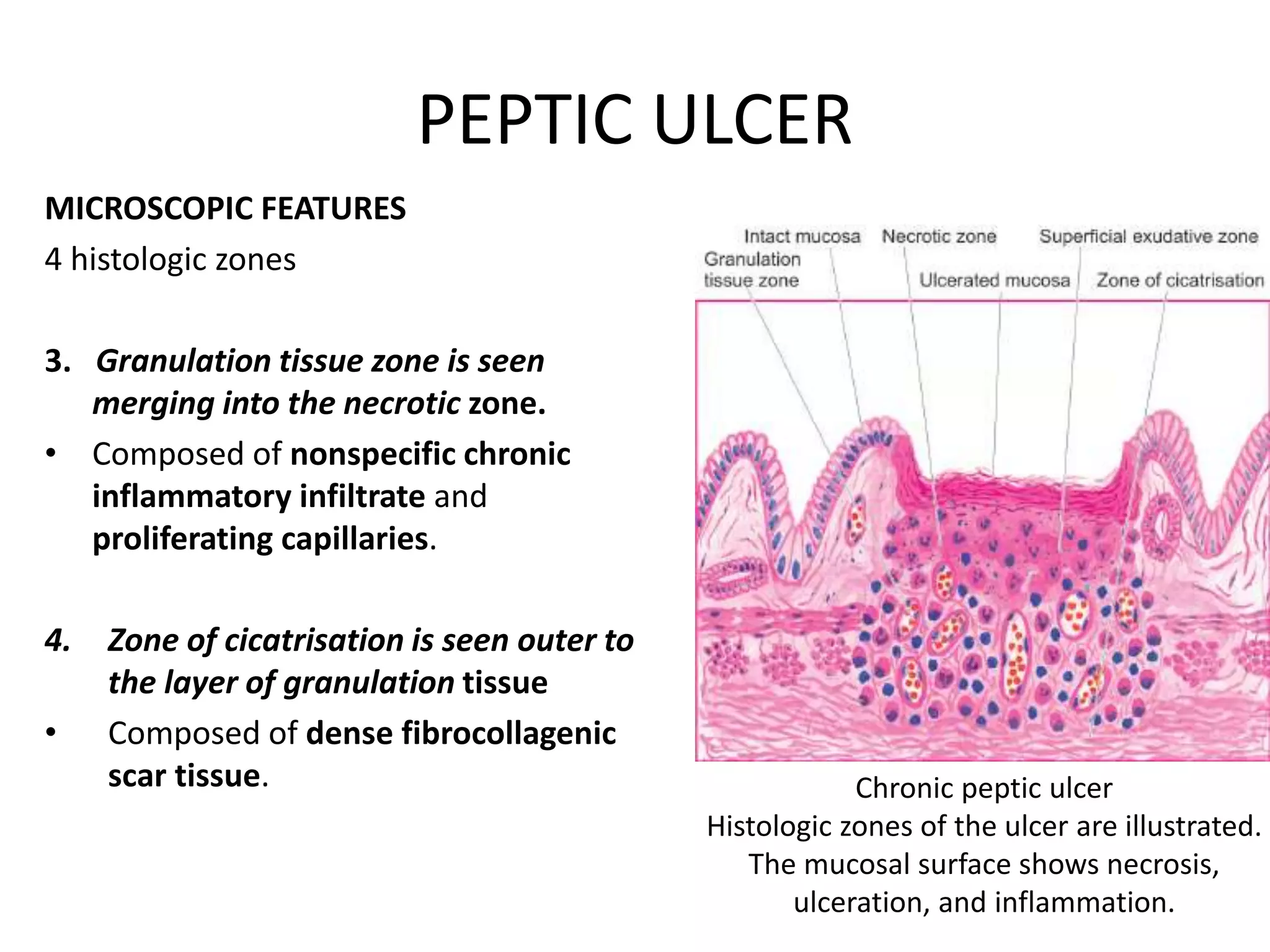





This document discusses the pathology of gastrointestinal tract lesions. It describes the gross and microscopic features of peptic ulcers, carcinoma of the stomach, and carcinoma of the colon. For peptic ulcers, it outlines the four histologic zones seen microscopically. For carcinoma of the stomach, it notes the common flat, infiltrating growth pattern and varying degrees of tumor cell differentiation. Carcinoma of the colon is described as having a right-sided fungating growth pattern or left-sided napkin ring configuration microscopically.
















































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)





