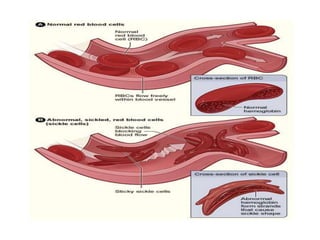
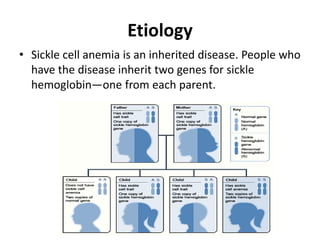
This document discusses hematological disorders involving red blood cells, including anemia and polycythemia. It defines different types of anemia such as iron deficiency anemia, pernicious anemia, and sickle cell anemia. For each type it discusses causes, signs and symptoms, diagnosis, treatment, and nursing considerations. It also covers polycythemia vera, defining it as a disorder where the bone marrow produces too many red blood cells, and discusses its pathophysiology, diagnostic tests, and treatment options.