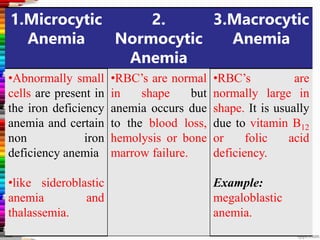
This document provides information about anaemia, including its definition, classification, causes, symptoms and treatment. It defines anaemia as a reduction in red blood cells or haemoglobin below the normal range. Anaemia can be classified based on red blood cell morphology (microcytic, normocytic, macrocytic) or etiology (blood loss, impaired production, increased destruction). Common causes include iron deficiency, vitamin B12/folate deficiency, sickle cell disease, aplastic anaemia, and haemolytic anaemia. Symptoms vary depending on the type but can include fatigue, pale skin, shortness of breath. Treatment depends on the underlying cause but may include iron supplementation, vitamin supplements, blood transfusions, and




























































































































![BLOOD_DISORDERS-2[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/blooddisorders-21-230610142333-f4472c75-thumbnail.jpg?width=640&height=640&fit=bounds)





























