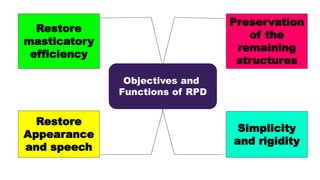
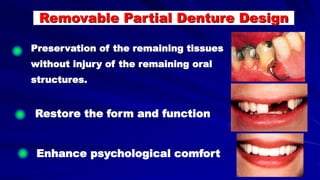
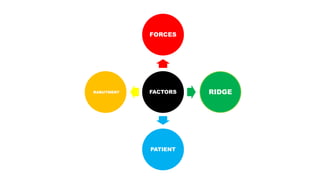
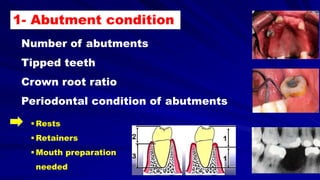
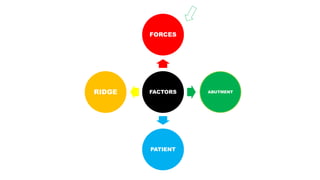
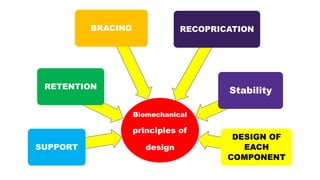
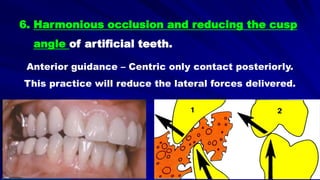
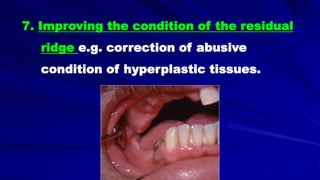
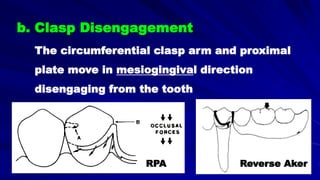
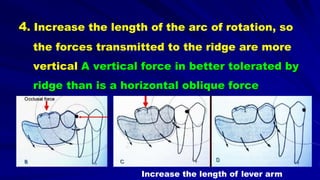
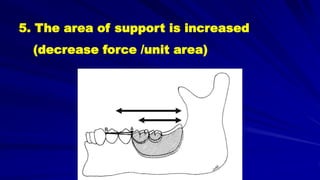
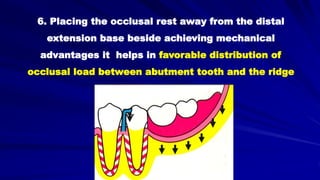
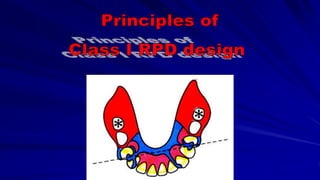
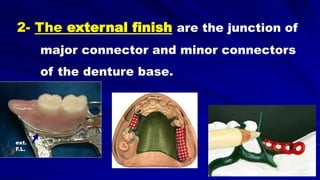
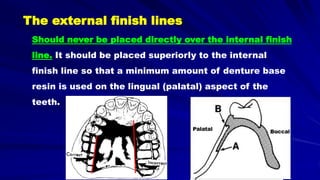
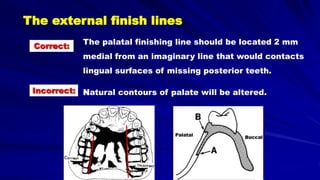
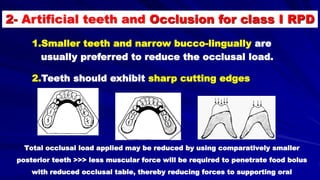
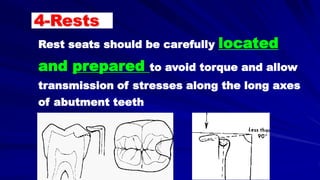
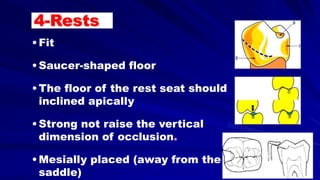
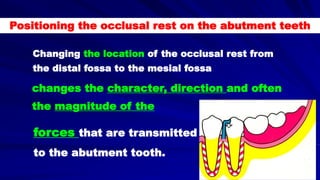
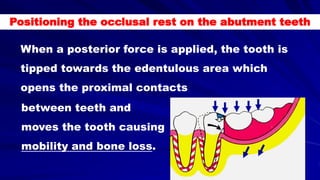
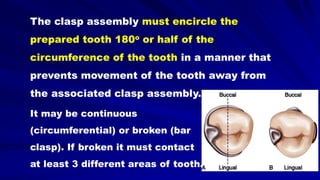
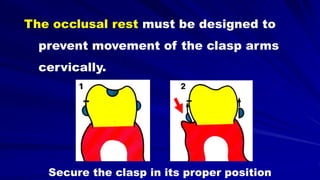
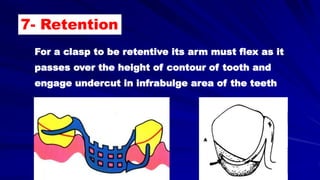
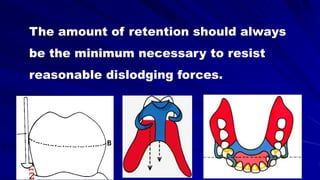
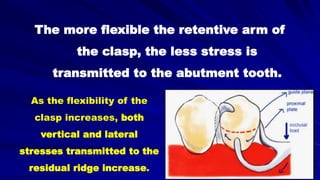
This document discusses the principles and factors involved in the design of removable partial dentures (RPDs) to ensure their effectiveness and minimize damage to dental structures. Key considerations include the health of abutment teeth, ridge conditions, and the biomechanical principles that guide the planning and alignment of the dentures. The aim is to achieve a secure and functional design that preserves existing tissues and supports masticatory efficiency while addressing the unique needs of patients.