
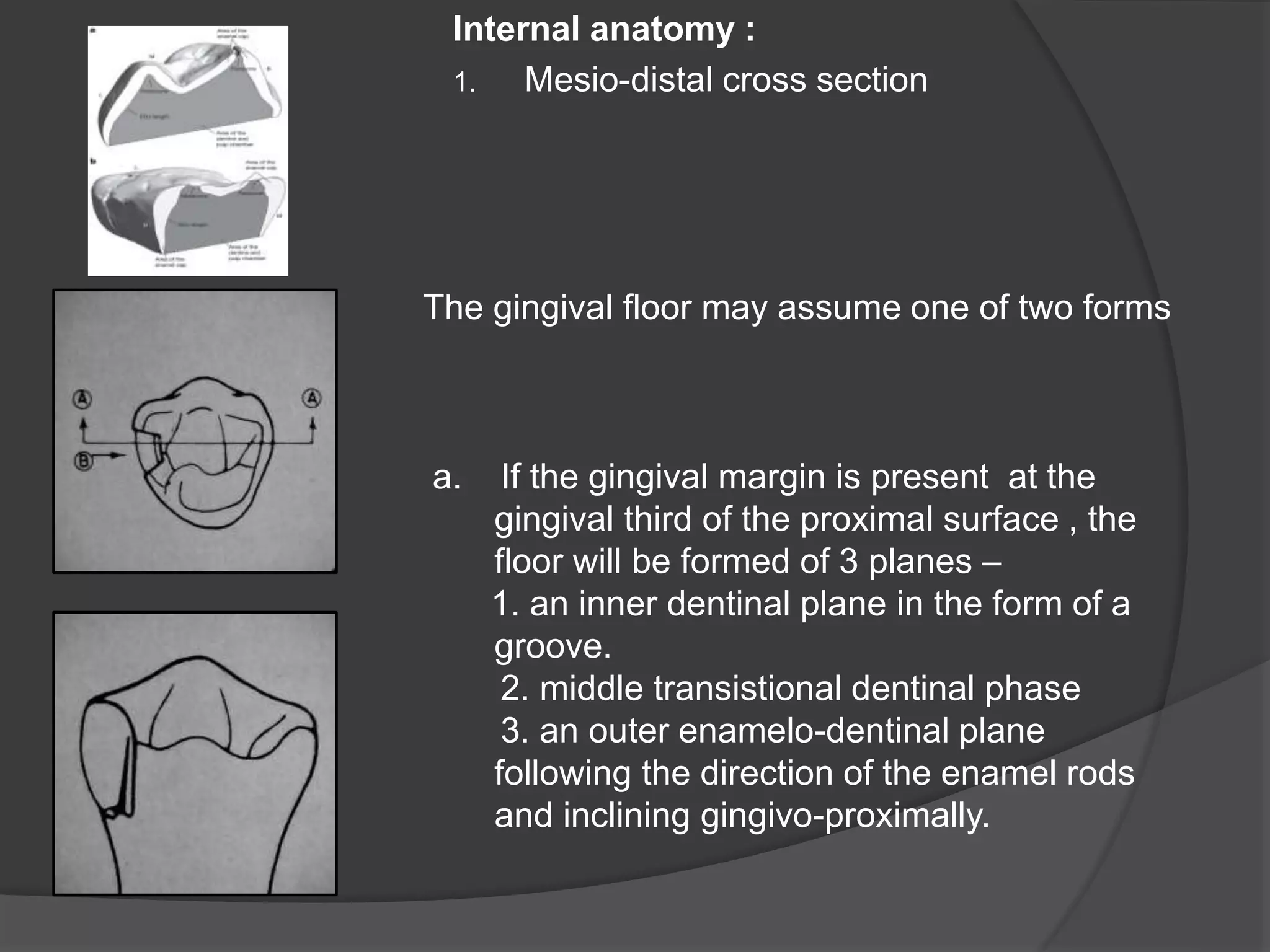
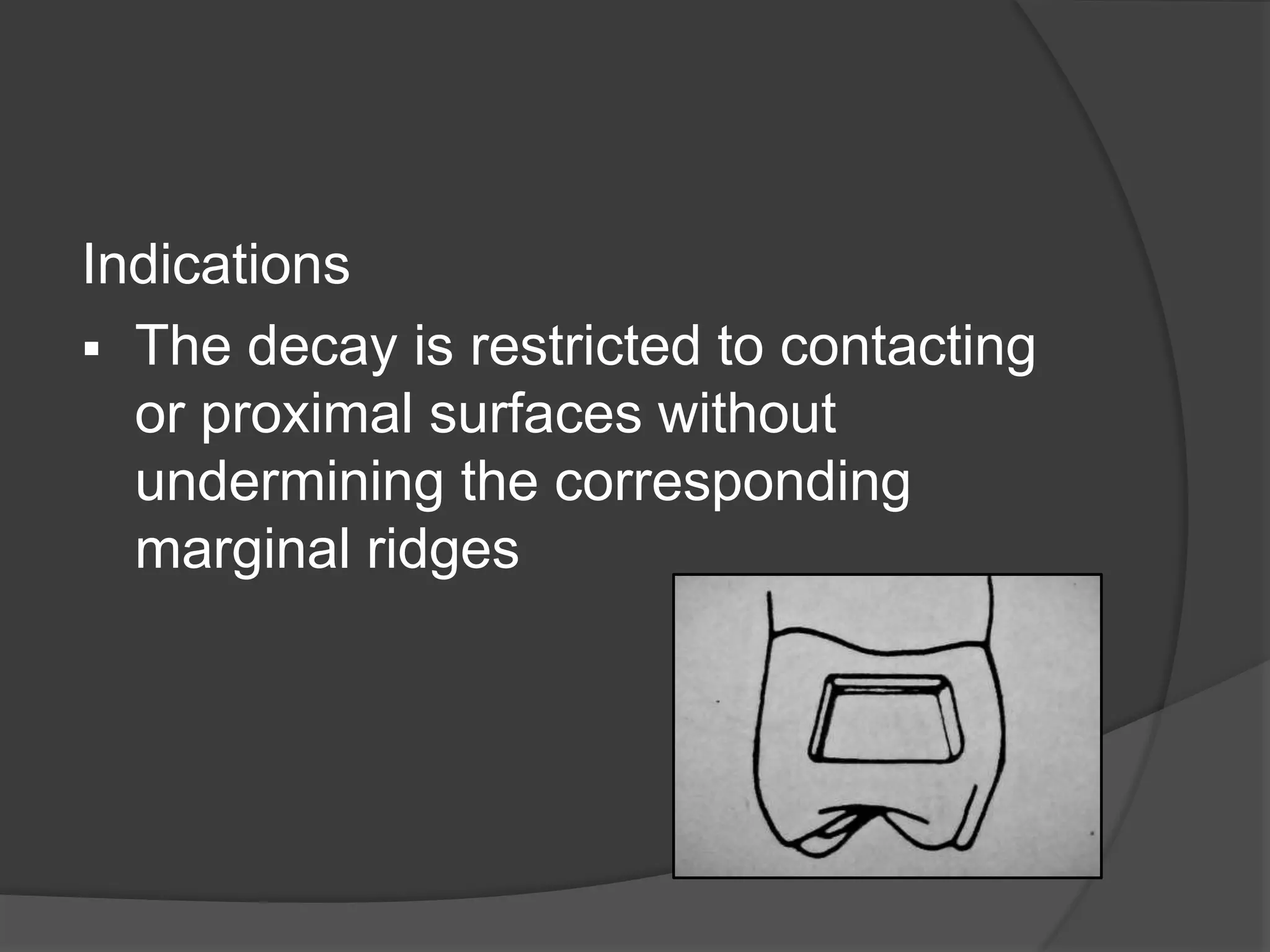
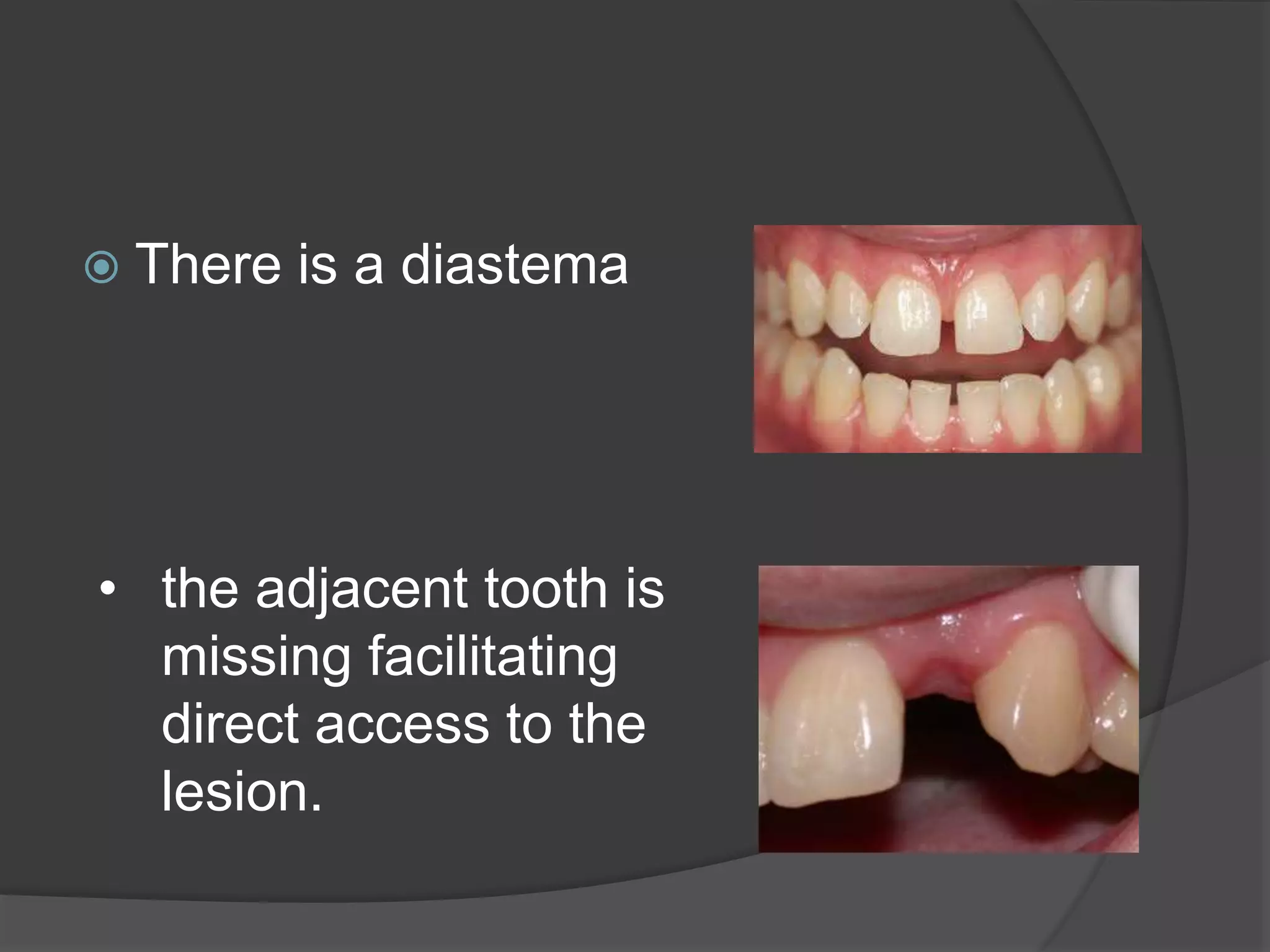
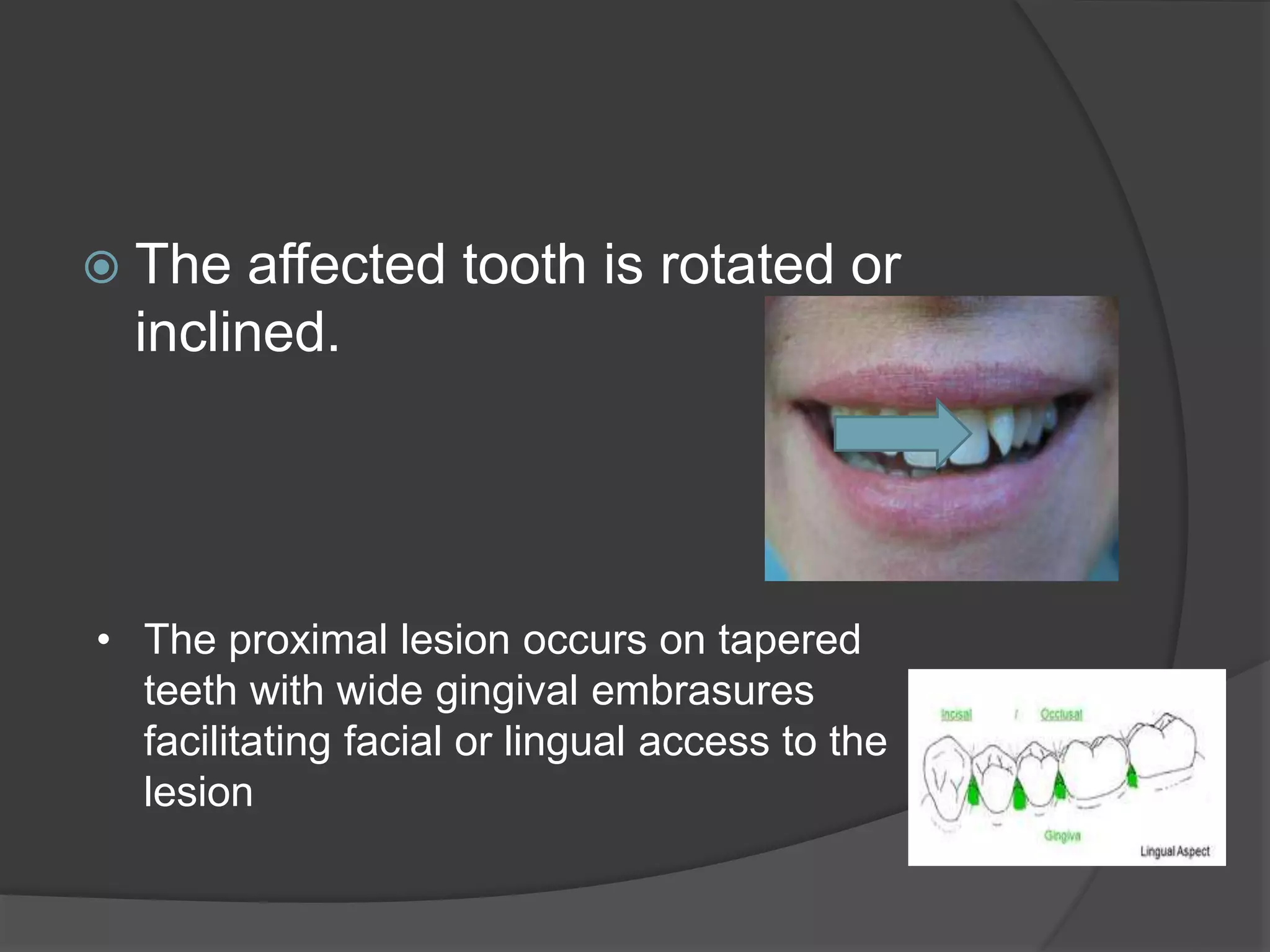
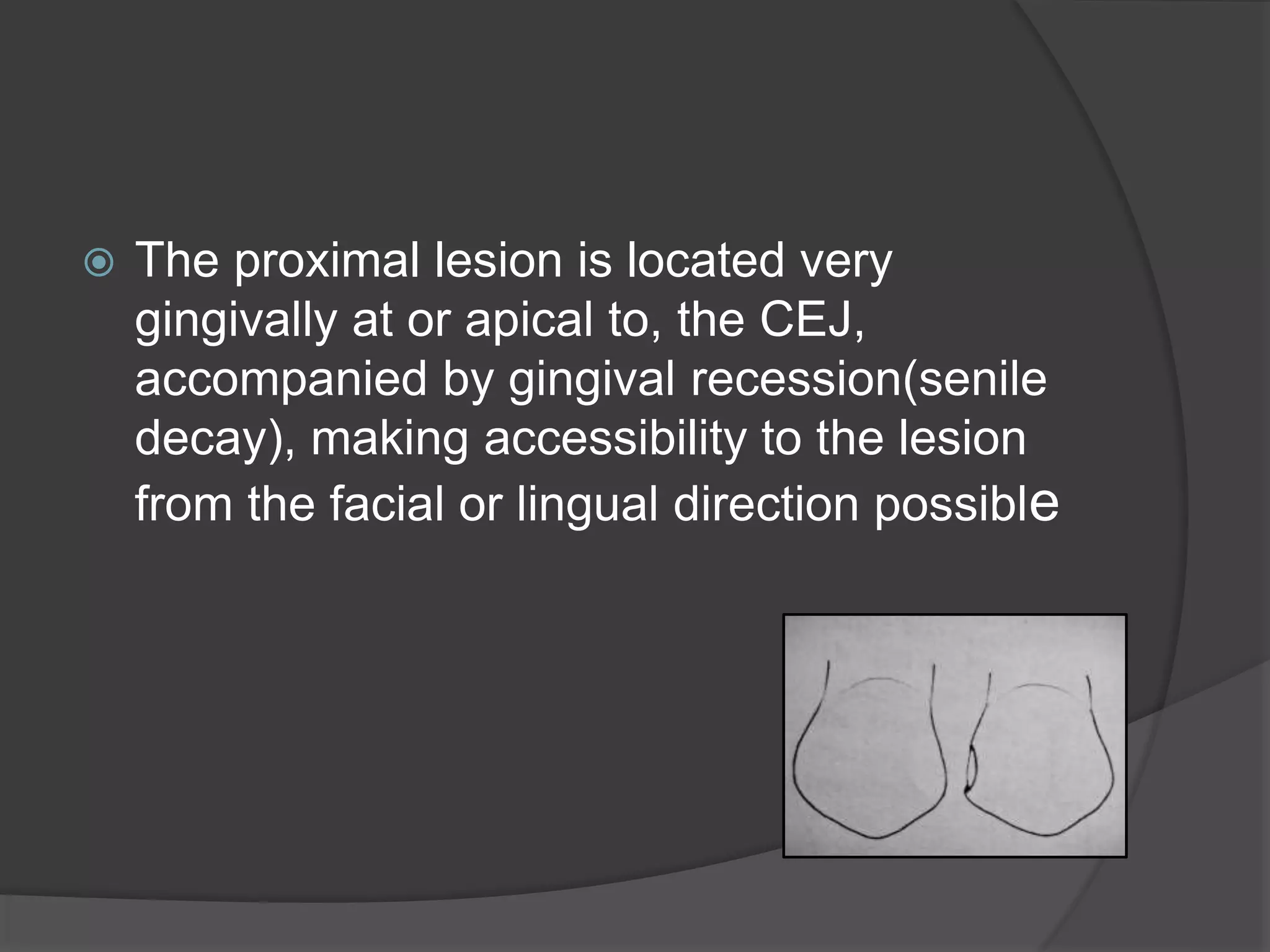

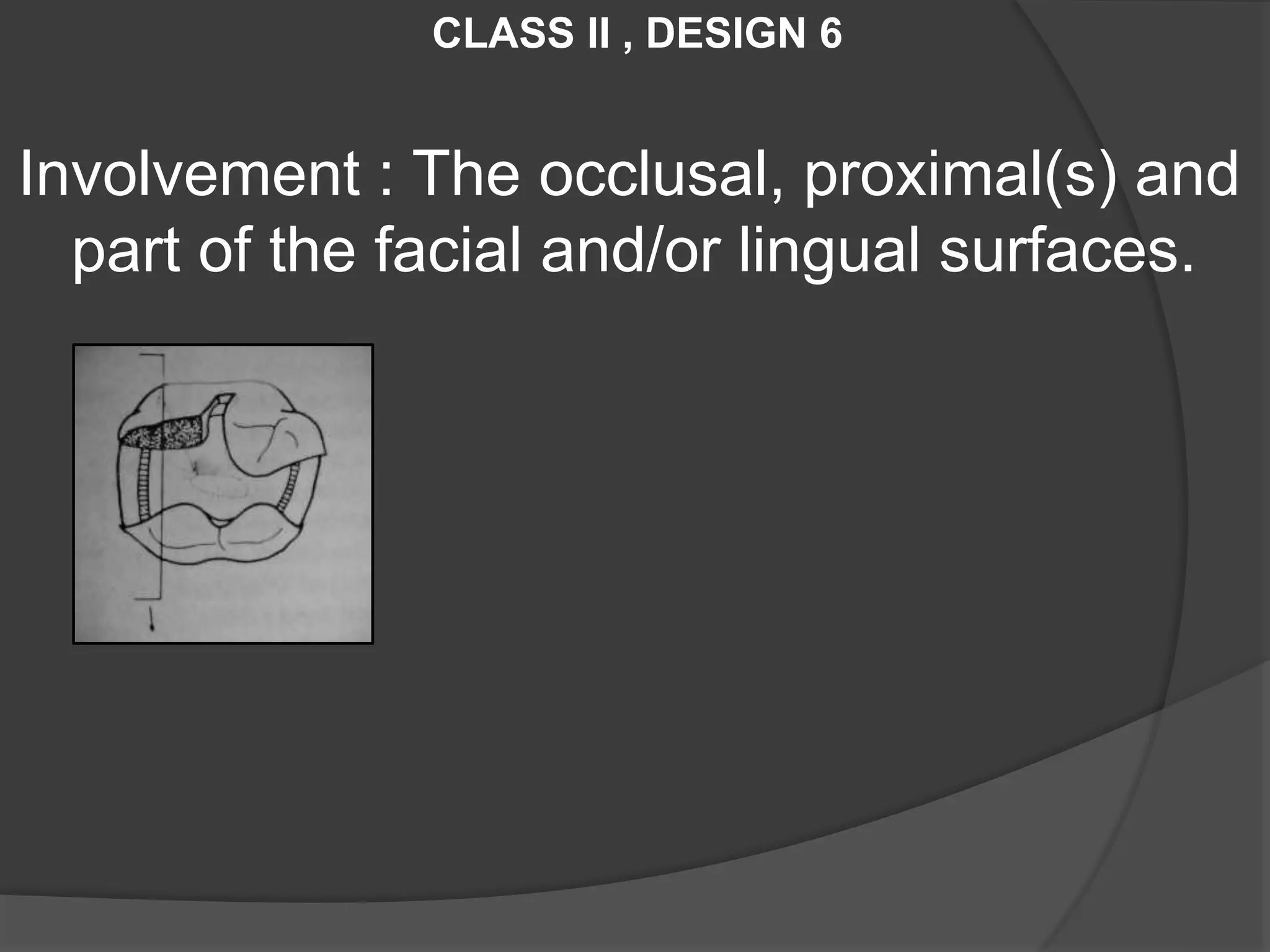
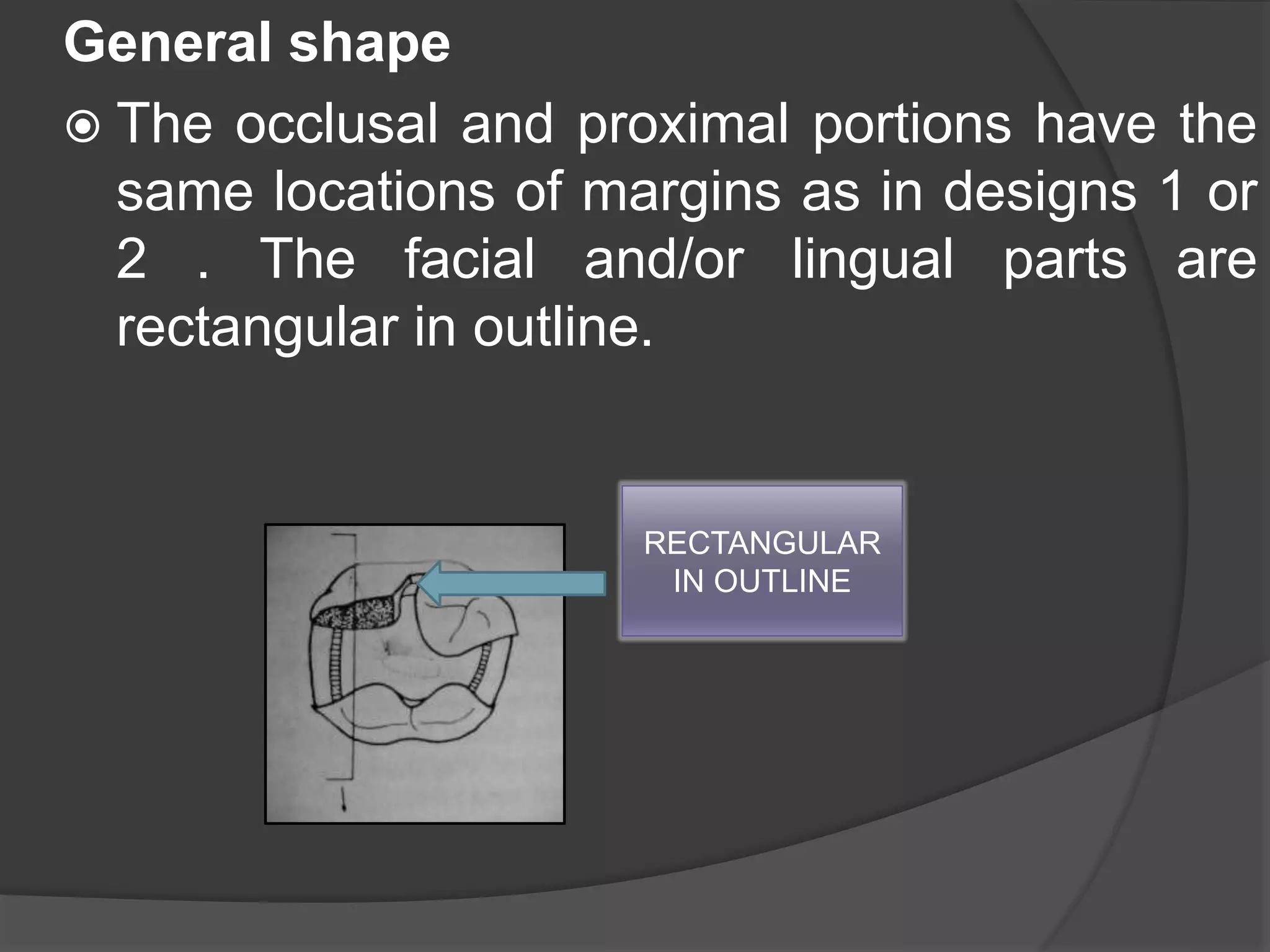
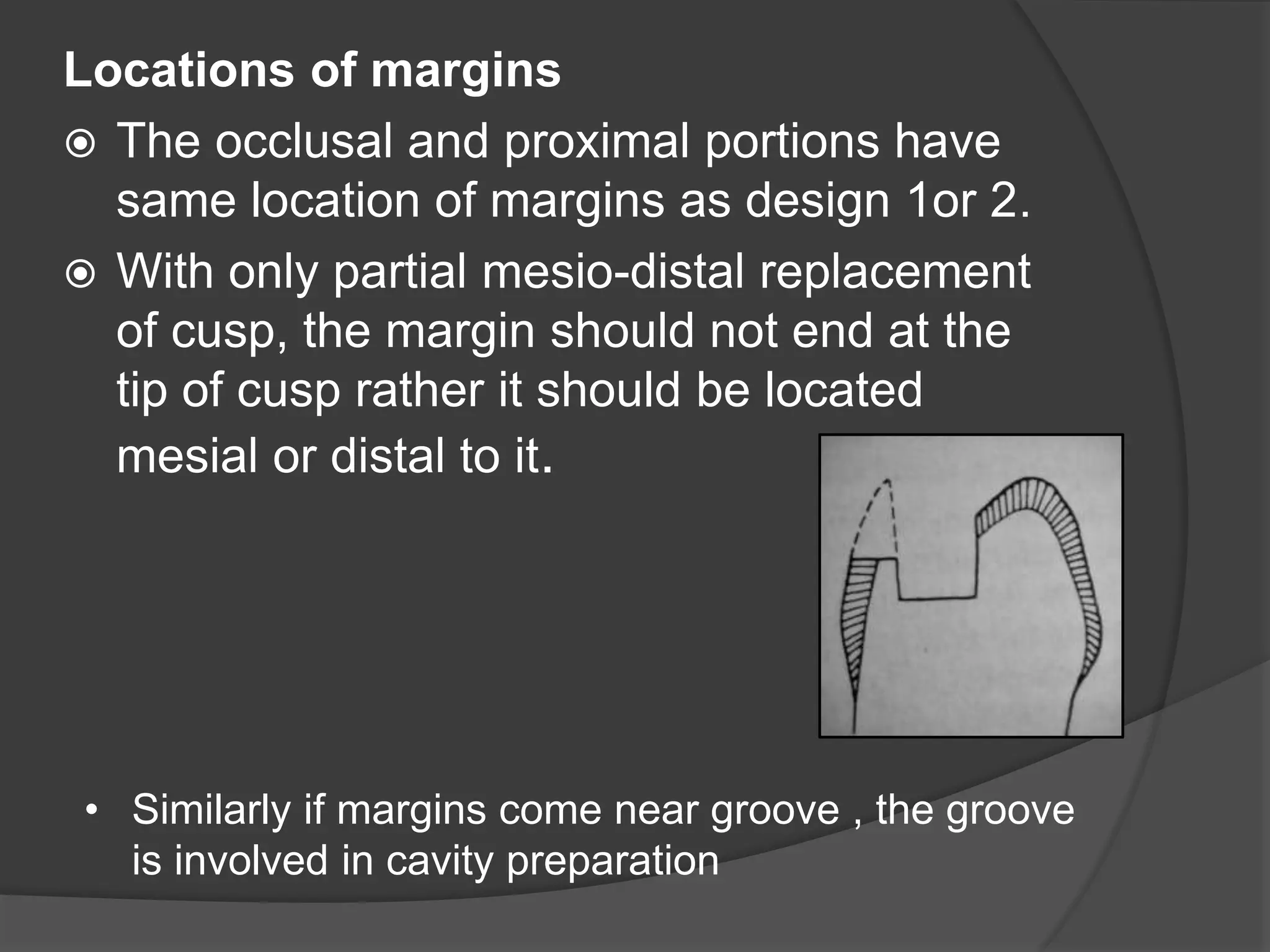

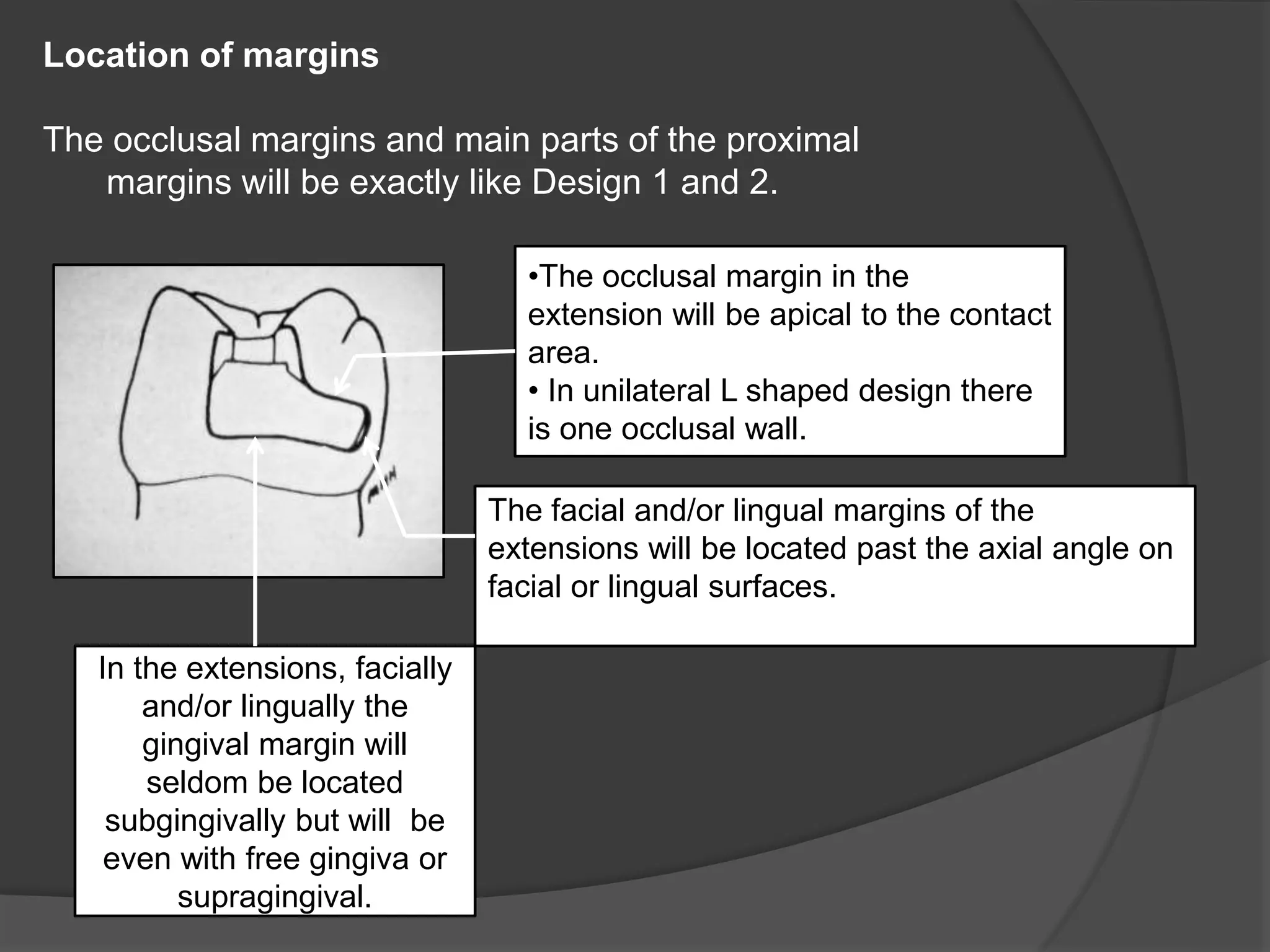
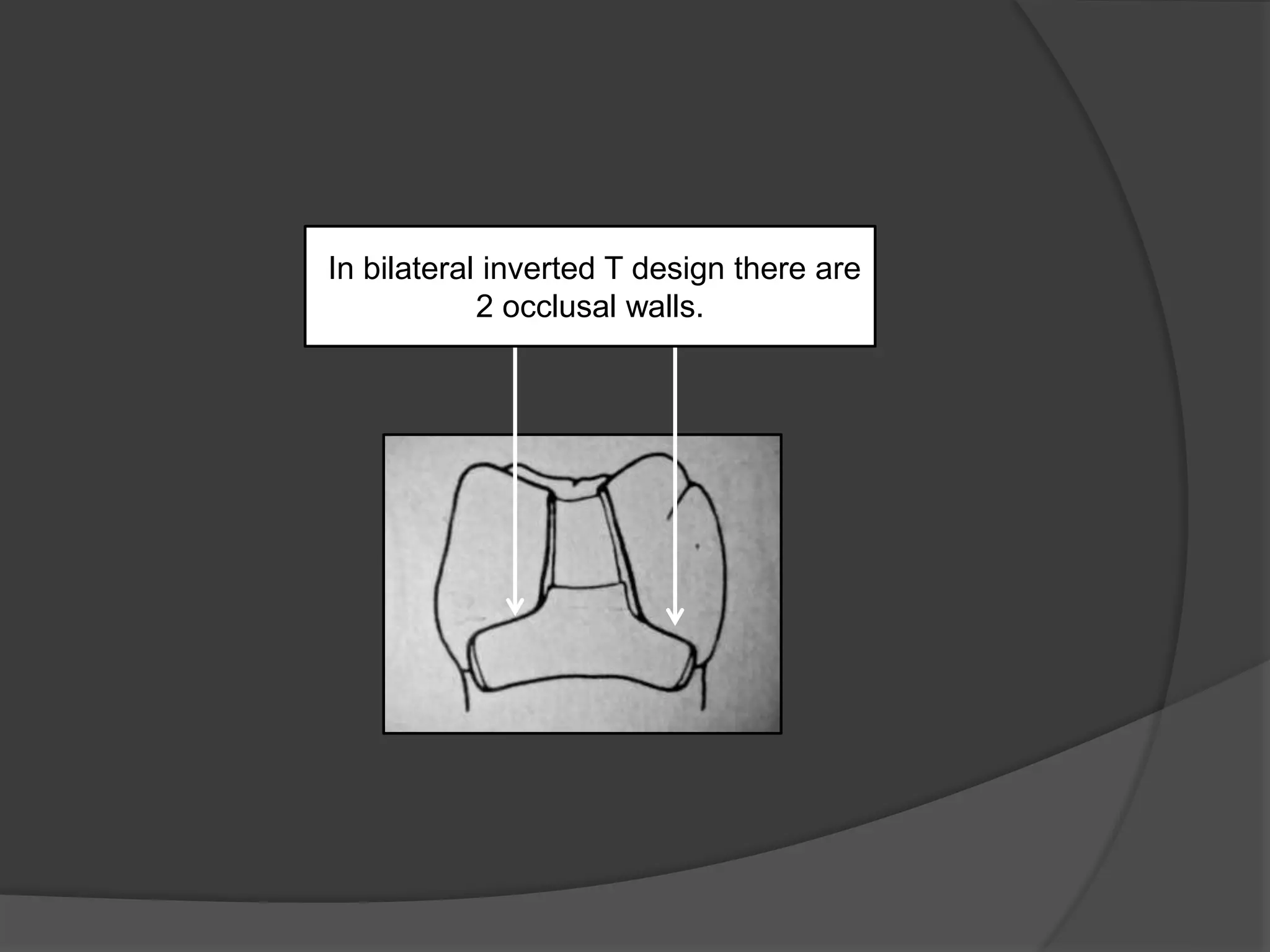
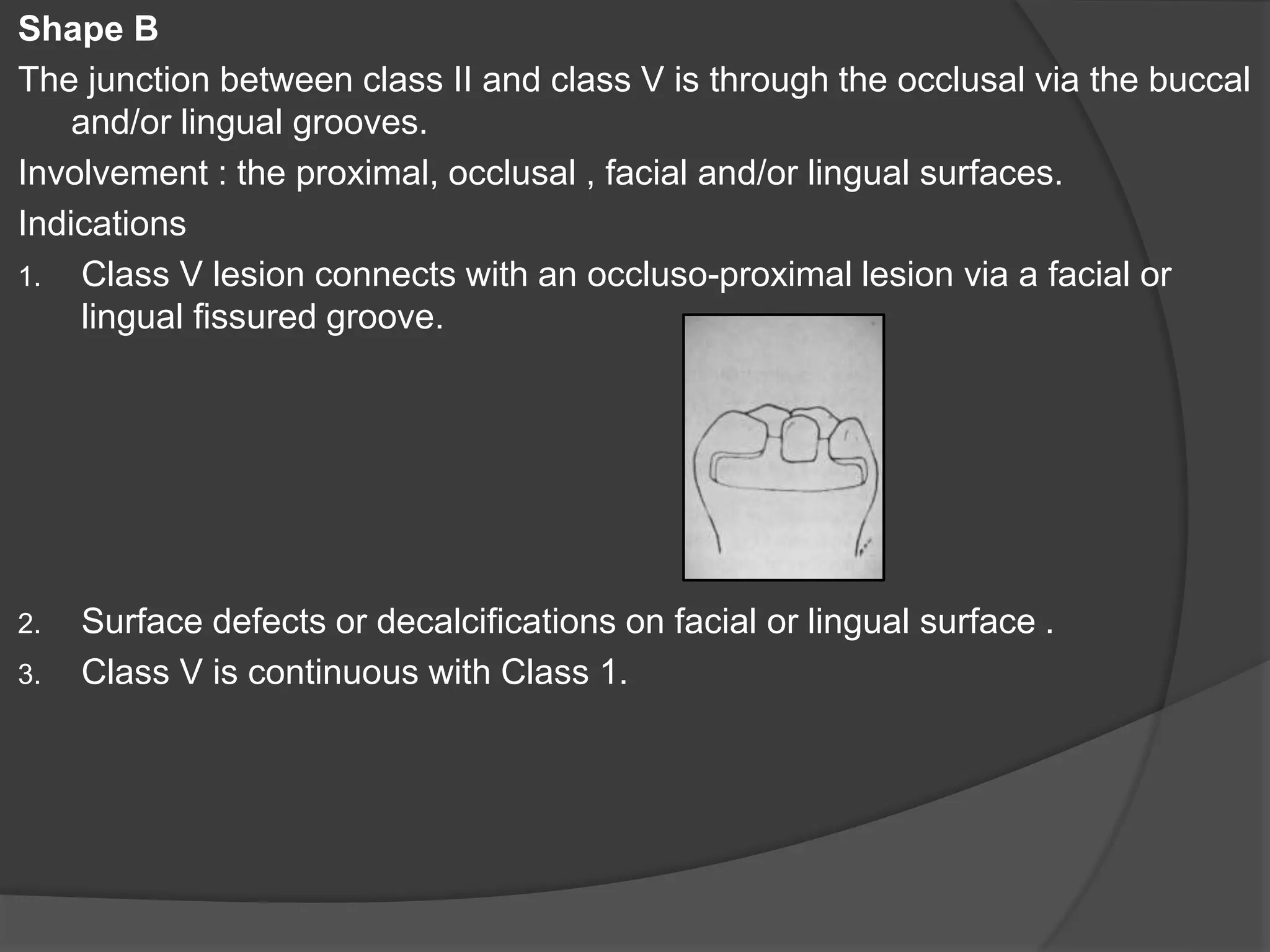
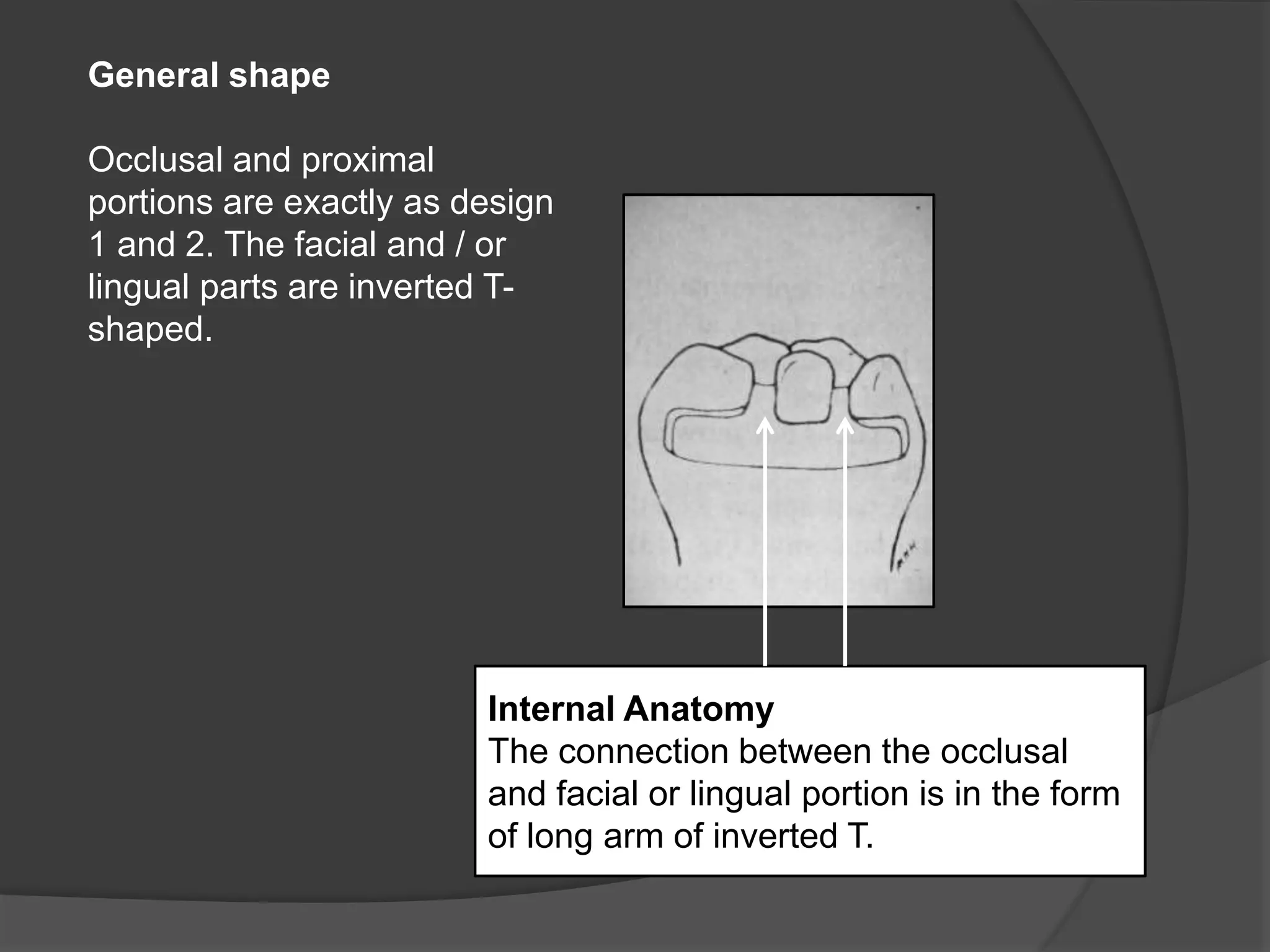

1) The document describes modifications to a standard Class 2 cavity preparation design based on factors like lesion size and location, tooth structure, and patient oral hygiene. 2) It presents 6 designs (labeled 1-6) that vary the cavity shape, locations of margins, and internal anatomy features to best suit different clinical situations. 3) Each design is indicated for specific caries patterns and locations, and involves different areas of the tooth structure, with variations in how the cavity preparation margins and walls are formed.























































































