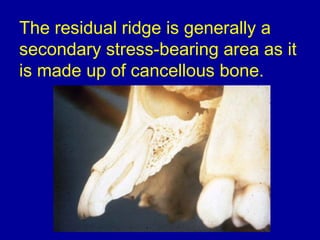
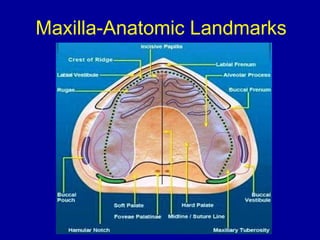
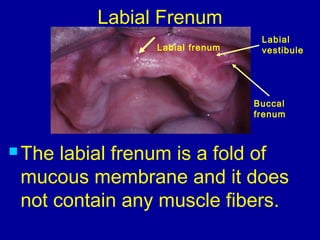
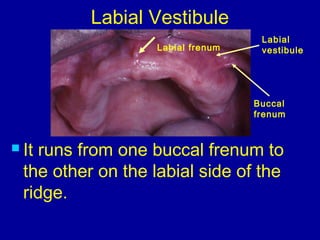
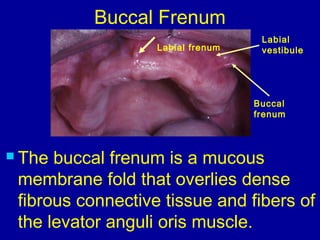
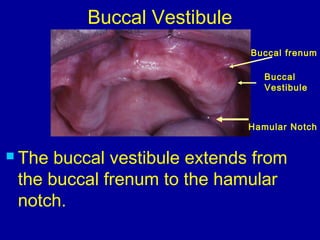
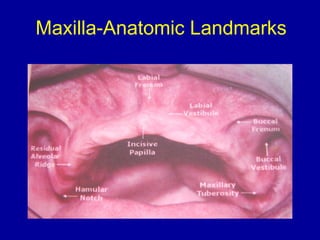
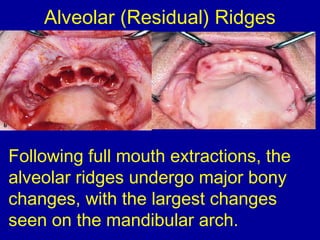
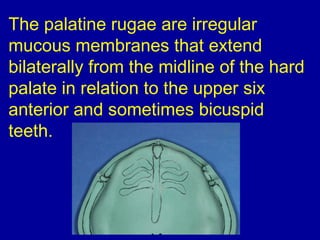
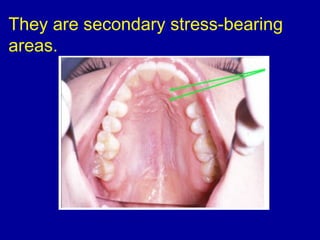
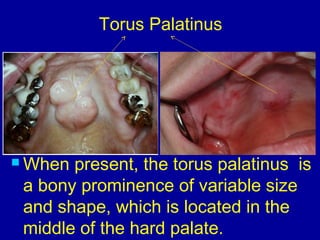
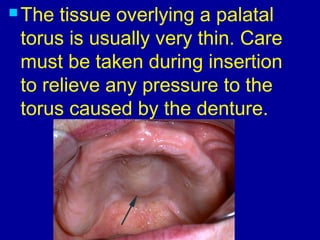
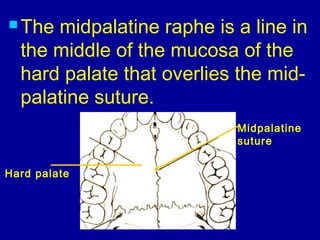
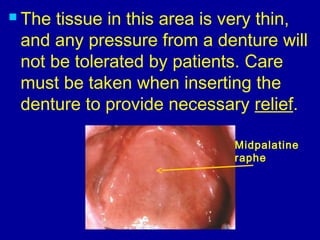
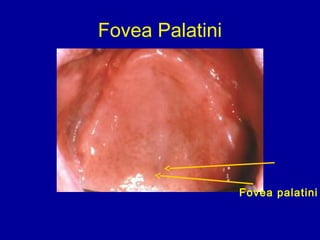
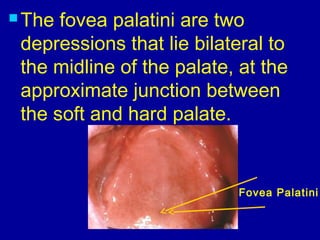
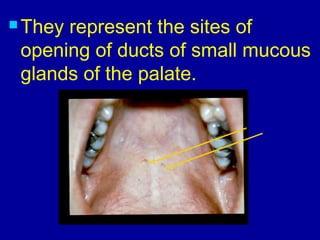
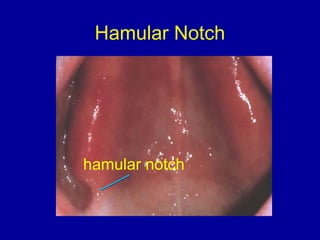
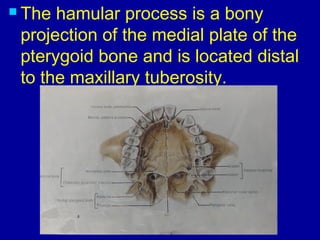
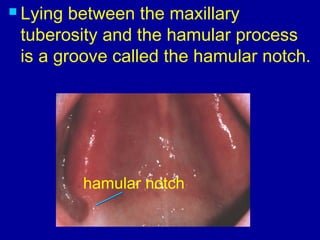
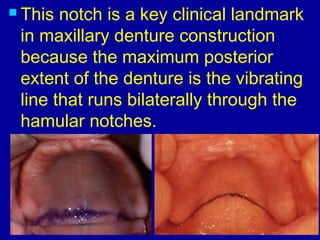
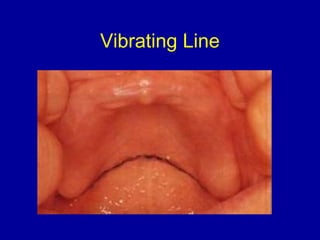
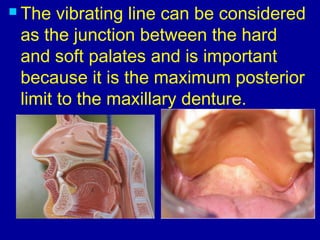
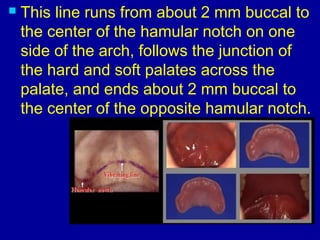
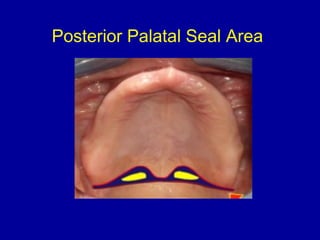
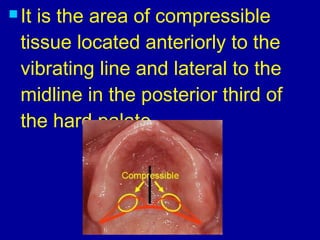
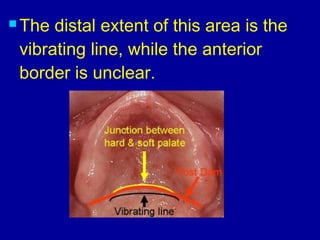
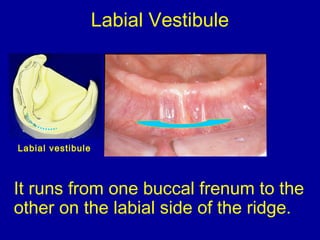
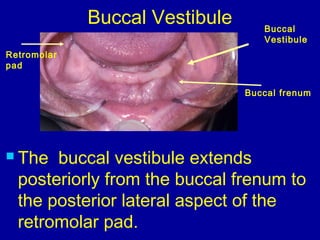
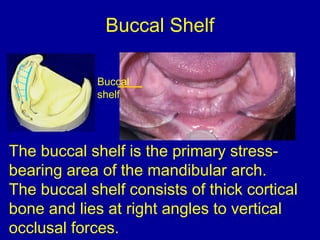
This document describes important anatomical landmarks in the edentulous maxilla and mandible that are relevant to complete denture prosthodontics. It defines relief areas, support areas, and stress bearing areas. For the maxilla, it identifies landmarks like the labial and buccal frenums, labial and buccal vestibules, alveolar ridges, maxillary tuberosity, incisive papilla, palatine rugae, torus palatinus, midpalatine raphe, fovea palatini, hamular notch, vibrating line, and posterior palatal seal area. For the mandible, it identifies landmarks like the labial and buccal frenums



















































![Anatomical landmarks of maxilla and mandible [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/anatomicallandmarksofmaxillaandmandibleautosaved-200820132830-thumbnail.jpg?width=640&height=640&fit=bounds)






















































