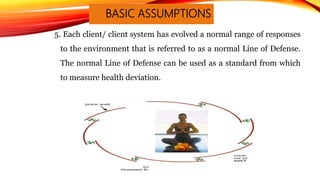
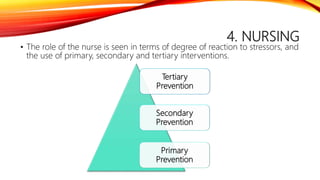
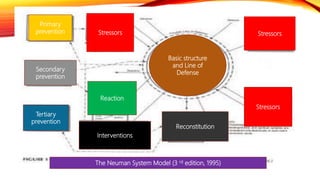
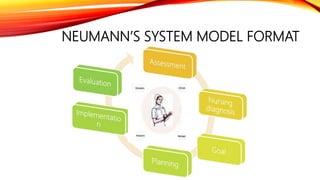
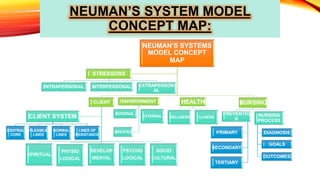
Betty Neumann's System Model provides a holistic framework for nursing focusing on how clients respond to stressors. It views clients as unique systems composed of physiological, psychological, socio-cultural, developmental, and spiritual subsystems that interact with internal and external environments. The model emphasizes primary, secondary, and tertiary prevention to help clients maintain wellness in response to stressors and regain stability if needed.