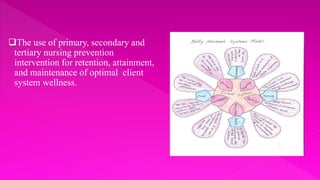
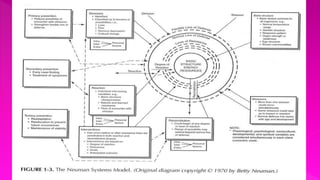
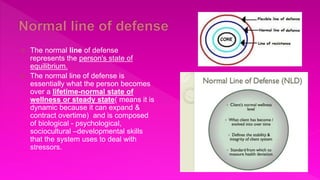

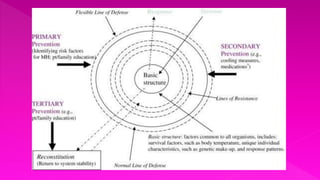
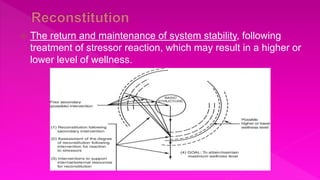



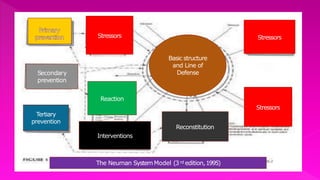

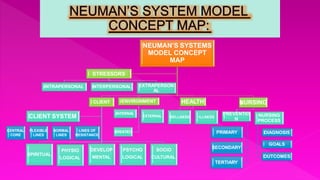


This document provides an overview of Betty Neumann's nursing theory and systems model. Some key points: - Neumann developed her systems model in the 1960s to provide nursing students with a holistic framework for understanding client problems. The model views each individual as a unique, open system interacting with the environment. - It focuses on a client's reaction to stressors and factors that promote reconstitution or adaptation. The model depicts concentric circles representing lines of defense that protect a client's basic structure from stressors. - Nursing aims to promote client stability through primary, secondary, and tertiary prevention interventions targeting stressors before, during, and after a reaction occurs. - The theory emphasizes viewing clients holistically
























































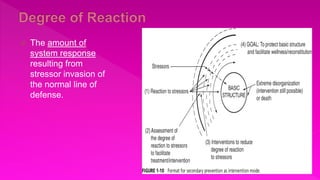
![Revised Topic- Schizophrenia [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/schizophreniaautosaved-250310073514-5d1607b2-thumbnail.jpg?width=640&height=640&fit=bounds)





![Revised -ppt of child psychiatric problems [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pptofchildpsychiatricproblemsautosaved-240926091227-d0592556-thumbnail.jpg?width=640&height=640&fit=bounds)























