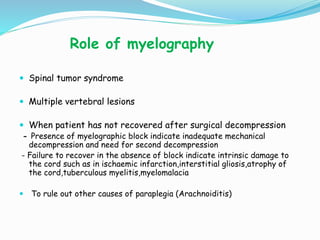
This document discusses the surgical management and approaches for spinal tuberculosis. Key points include:
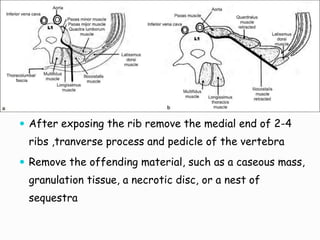
- Surgical management includes debridement of diseased vertebrae, drainage of abscesses, arthrodesis for instability, and decompression for neurological complications.
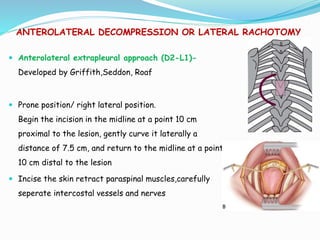
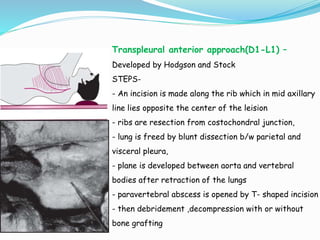
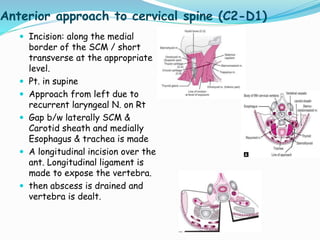
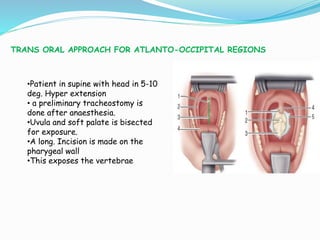
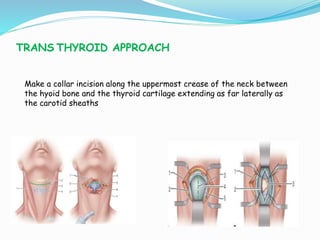
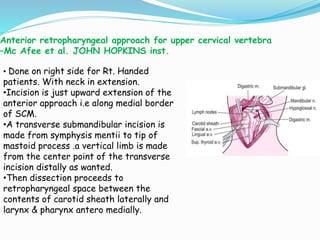
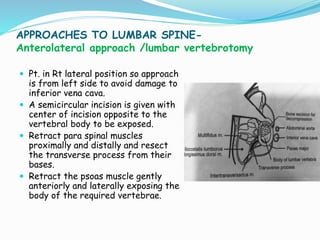
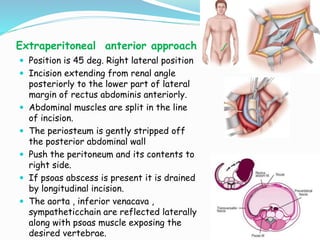
- Common surgical approaches discussed for different spinal regions include anterior, posterior, anterolateral, costotransversectomy, and laminectomy.
- Indications for surgery include neurological deficits not improving with conservative treatment, mechanical instability, and prevention of severe kyphosis.



































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






